Physician Additional 2018-2026


What is the Physician Additional?
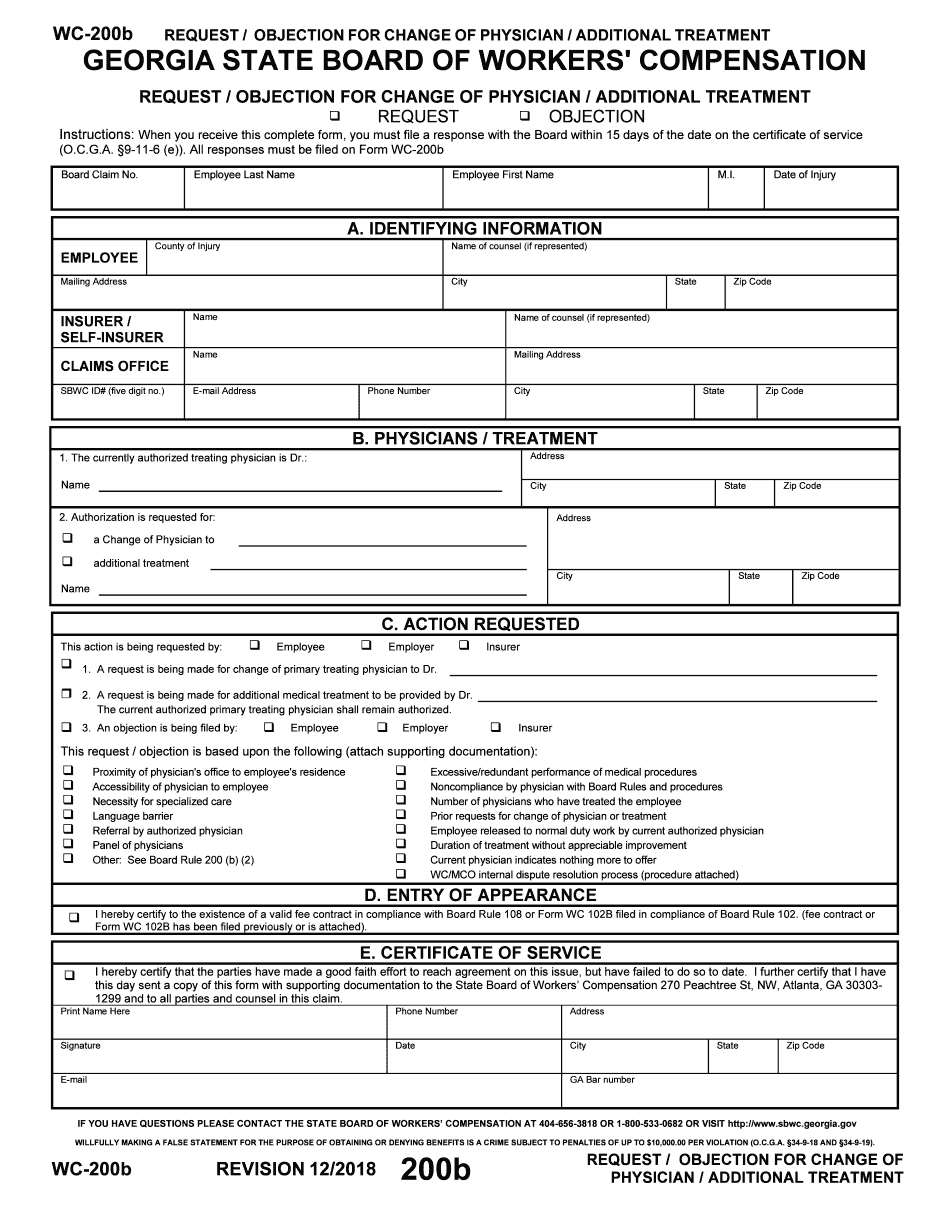
The Physician Additional is a specific form used in the state of Georgia to request additional medical treatment related to a workers' compensation claim. This form, often referred to as the Georgia form WC 200B, is essential for individuals seeking to modify their treatment plan or address any changes in their medical care. It serves as an official request to ensure that the necessary medical services are provided and documented appropriately within the context of workers' compensation regulations.
How to Use the Physician Additional
To effectively use the Physician Additional, individuals must first complete the form accurately, detailing the required information regarding their medical condition and the specific treatments being requested. It is important to include any relevant medical documentation that supports the need for additional treatment. Once completed, the form should be submitted to the appropriate workers' compensation board or insurance provider to initiate the review process. Ensuring that all sections are filled out clearly will facilitate a smoother approval process.
Steps to Complete the Physician Additional
Completing the Physician Additional involves several key steps:
- Gather all necessary medical records and documentation related to your current treatment.
- Fill out the form with accurate personal and medical information.
- Clearly specify the additional treatment being requested and the rationale behind it.
- Review the form for completeness and accuracy before submission.
- Submit the completed form to the relevant authority, either online or via mail.
Required Documents
When submitting the Physician Additional, it is crucial to include supporting documents that substantiate the request for additional treatment. These documents may include:
- Medical records from treating physicians.
- Previous treatment plans and outcomes.
- Any diagnostic tests or evaluations that support the need for further treatment.
Legal Use of the Physician Additional
The Physician Additional is legally recognized within the framework of Georgia's workers' compensation laws. It is essential to ensure that the form is filled out in compliance with these regulations to avoid any potential legal issues. Proper use of this form can help secure necessary medical treatment and protect the rights of the injured worker under state law.
Form Submission Methods
The Physician Additional can be submitted through various methods, depending on the requirements of the workers' compensation board or insurance provider. Common submission methods include:
- Online submission via the designated workers' compensation portal.
- Mailing the completed form to the appropriate office.
- In-person delivery to the local workers' compensation office.
Quick guide on how to complete request objection for change of physician additional treatment wc 200b
Complete Physician Additional seamlessly on any device
Digital document management has gained popularity among both organizations and individuals. It offers an ideal eco-friendly alternative to conventional printed and signed documents, allowing you to obtain the necessary form and securely store it online. airSlate SignNow provides you with all the resources required to create, edit, and eSign your documents swiftly and without hitches. Manage Physician Additional on any platform using airSlate SignNow’s Android or iOS applications and enhance any document-related process today.
How to edit and eSign Physician Additional with ease
- Locate Physician Additional and click on Retrieve Form to begin.
- Utilize the tools we offer to finalize your document.
- Mark relevant sections of the documents or obscure sensitive information with tools that airSlate SignNow provides specifically for that purpose.
- Generate your eSignature using the Sign tool, which takes mere seconds and has the same legal validity as a conventional wet ink signature.
- Verify the details and click on the Complete button to store your modifications.
- Select your preferred delivery method for your form, whether it’s via email, SMS, invitation link, or downloading it to your computer.
No more worrying about lost or misfiled documents, tedious form searches, or mistakes that necessitate printing additional document copies. airSlate SignNow fulfills your document management needs in just a few clicks from any device of your choice. Edit and eSign Physician Additional and ensure outstanding communication at every stage of the form preparation process with airSlate SignNow.
Create this form in 5 minutes or less
Create this form in 5 minutes!
How to create an eSignature for the request objection for change of physician additional treatment wc 200b
How to make an electronic signature for your Request Objection For Change Of Physician Additional Treatment Wc 200b online
How to generate an eSignature for your Request Objection For Change Of Physician Additional Treatment Wc 200b in Google Chrome
How to create an eSignature for signing the Request Objection For Change Of Physician Additional Treatment Wc 200b in Gmail
How to generate an electronic signature for the Request Objection For Change Of Physician Additional Treatment Wc 200b right from your smartphone
How to make an eSignature for the Request Objection For Change Of Physician Additional Treatment Wc 200b on iOS devices
How to make an eSignature for the Request Objection For Change Of Physician Additional Treatment Wc 200b on Android
People also ask
-
What is the process to GA change physician using airSlate SignNow?
To GA change physician using airSlate SignNow, simply log in to your account and navigate to the document requiring the update. You can easily edit the relevant sections to reflect the new physician's information and send it for electronic signing. The process is quick, ensuring that your document remains compliant and up-to-date.
-
How much does it cost to use airSlate SignNow for GA change physician?
airSlate SignNow offers flexible pricing plans starting with a free trial. Depending on the features you choose, the monthly costs can vary, providing great value for handling GA change physician electronically and efficiently. You can select a plan that fits your business needs without breaking the bank.
-
What features does airSlate SignNow offer for GA change physician?
airSlate SignNow provides robust features for GA change physician, including customizable templates, electronic signatures, and real-time document tracking. These tools streamline the updating process, making your document management simpler and more effective, especially in healthcare settings.
-
How does airSlate SignNow assist in maintaining compliance during GA change physician?
With airSlate SignNow, you can maintain compliance during GA change physician by utilizing templates that adhere to legal standards. The platform ensures that all signatures are secure and verifiable while also keeping an audit trail for future reference, which is particularly important in healthcare.
-
Can I integrate airSlate SignNow with other systems for GA change physician?
Yes, airSlate SignNow seamlessly integrates with various third-party applications to enhance your workflows, especially when handling GA change physician. You can connect it with CRM systems, cloud storage, and more, ensuring that your document management aligns well with your existing processes.
-
What are the benefits of using airSlate SignNow for GA change physician?
Using airSlate SignNow for GA change physician brings numerous benefits, such as improved efficiency, reduced paperwork, and faster turnaround times for document signing. Organizations can easily manage changes while focusing on patient care rather than administrative hurdles.
-
Is it easy to use airSlate SignNow for GA change physician for first-time users?
Absolutely! airSlate SignNow is designed to be user-friendly, making it straightforward for first-time users to GA change physician. The intuitive interface guides you through each step, and ample online resources and support are available to ensure a smooth user experience.
Get more for Physician Additional
- Employee code of conduct pdf form
- Alankit tpa hospital empanelment form
- Bank of america signature card form
- The law of attraction book by mitesh khatri pdf download form
- Air india medical form
- Mdcps formal grevience
- Our move out form accel property management amp investments llc
- Brand identity contract template form
Find out other Physician Additional
- How To eSign South Dakota Plumbing Quitclaim Deed
- How To eSign South Dakota Plumbing Affidavit Of Heirship
- eSign South Dakota Plumbing Emergency Contact Form Myself
- eSign Texas Plumbing Resignation Letter Free
- eSign West Virginia Orthodontists Living Will Secure
- Help Me With eSign Texas Plumbing Business Plan Template
- Can I eSign Texas Plumbing Cease And Desist Letter
- eSign Utah Plumbing Notice To Quit Secure
- eSign Alabama Real Estate Quitclaim Deed Mobile
- eSign Alabama Real Estate Affidavit Of Heirship Simple
- eSign California Real Estate Business Plan Template Free
- How Can I eSign Arkansas Real Estate Promissory Note Template
- eSign Connecticut Real Estate LLC Operating Agreement Later
- eSign Connecticut Real Estate LLC Operating Agreement Free
- eSign Real Estate Document Florida Online
- eSign Delaware Real Estate Quitclaim Deed Easy
- eSign Hawaii Real Estate Agreement Online
- Help Me With eSign Hawaii Real Estate Letter Of Intent
- eSign Florida Real Estate Residential Lease Agreement Simple
- eSign Florida Real Estate Limited Power Of Attorney Online