Patient S Request for Medical Payment Form


What is the Patient’s Request For Medical Payment
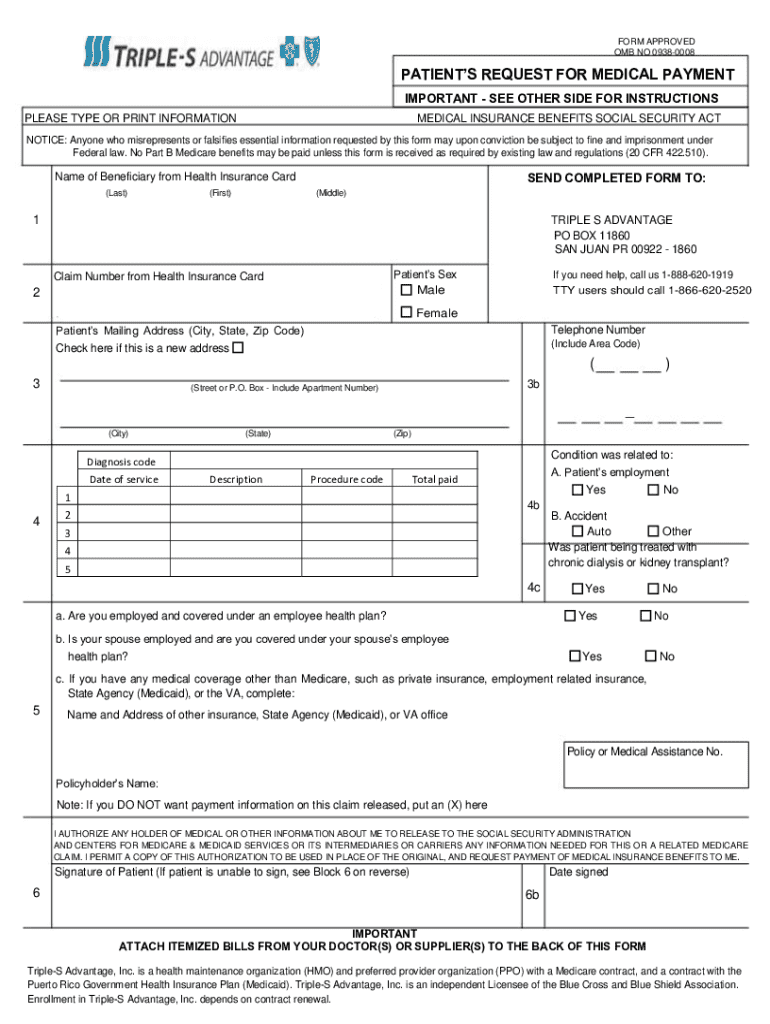
The Patient’s Request For Medical Payment is a formal document used by patients to request reimbursement for medical expenses incurred. This form is essential for patients seeking to claim payments from their health insurance providers or other entities responsible for covering medical costs. It typically includes details about the patient, the healthcare provider, the services rendered, and the associated costs. Understanding this form is crucial for ensuring that patients receive the financial support they are entitled to for their medical care.
How to use the Patient’s Request For Medical Payment
Using the Patient’s Request For Medical Payment involves a few straightforward steps. First, patients need to gather all relevant information, including personal details, insurance information, and documentation of medical services received. Next, they should accurately fill out the form, ensuring that all sections are completed to avoid delays in processing. After completing the form, patients must submit it to their insurance provider or the appropriate entity responsible for payment. Keeping a copy of the submitted form for personal records is also advisable.
Steps to complete the Patient’s Request For Medical Payment
Completing the Patient’s Request For Medical Payment involves several key steps:
- Collect necessary documents, such as medical bills, insurance cards, and any supporting paperwork.
- Fill out the form with accurate personal and insurance information.
- Detail the medical services received, including dates and costs.
- Sign and date the form to certify the information provided is accurate.
- Submit the form to the appropriate insurance company or payment entity.
Key elements of the Patient’s Request For Medical Payment
Several key elements must be included in the Patient’s Request For Medical Payment to ensure proper processing:
- Patient Information: Full name, address, and contact details.
- Insurance Information: Policy number and provider details.
- Provider Information: Name and contact details of the healthcare provider.
- Details of Services: Description of the medical services, including dates and costs.
- Signature: The patient’s signature certifying the accuracy of the information.
Legal use of the Patient’s Request For Medical Payment
The Patient’s Request For Medical Payment is a legally binding document that patients use to claim reimbursement for medical expenses. It is important for patients to ensure that all information provided is truthful and accurate, as any discrepancies can lead to delays or denial of claims. Additionally, this form may be subject to state-specific regulations, making it essential for patients to understand the legal implications of submitting this request in their respective states.
Form Submission Methods
Patients can submit the Patient’s Request For Medical Payment through various methods, including:
- Online Submission: Many insurance providers offer online portals for submitting claims electronically.
- Mail: Patients can print the completed form and send it via postal service to their insurance company.
- In-Person: Some patients may choose to deliver the form directly to their insurance provider’s office for immediate processing.
Create this form in 5 minutes or less
Create this form in 5 minutes!
How to create an eSignature for the patients request for medical payment
How to create an electronic signature for a PDF online
How to create an electronic signature for a PDF in Google Chrome
How to create an e-signature for signing PDFs in Gmail
How to create an e-signature right from your smartphone
How to create an e-signature for a PDF on iOS
How to create an e-signature for a PDF on Android
People also ask
-
What is a Patient’s Request For Medical Payment?
A Patient’s Request For Medical Payment is a formal document that patients use to request reimbursement for medical expenses. This process ensures that patients can efficiently manage their healthcare costs and receive timely payments. Utilizing airSlate SignNow simplifies this process by allowing users to create, send, and eSign these requests seamlessly.
-
How does airSlate SignNow streamline the Patient’s Request For Medical Payment process?
airSlate SignNow streamlines the Patient’s Request For Medical Payment process by providing an intuitive platform for document creation and electronic signatures. Users can easily customize templates, ensuring that all necessary information is included. This efficiency reduces the time spent on paperwork and accelerates the reimbursement process.
-
What are the pricing options for using airSlate SignNow for Patient’s Request For Medical Payment?
airSlate SignNow offers flexible pricing plans tailored to different business needs, including options for small practices and larger healthcare organizations. Each plan provides access to essential features for managing Patient’s Request For Medical Payment efficiently. You can choose a plan that best fits your budget and requirements.
-
Can airSlate SignNow integrate with other healthcare software for managing Patient’s Request For Medical Payment?
Yes, airSlate SignNow integrates seamlessly with various healthcare software systems, enhancing the management of Patient’s Request For Medical Payment. This integration allows for automatic data transfer and improved workflow efficiency. By connecting your existing tools, you can streamline the entire payment request process.
-
What features does airSlate SignNow offer for handling Patient’s Request For Medical Payment?
airSlate SignNow provides features such as customizable templates, secure eSigning, and real-time tracking for Patient’s Request For Medical Payment. These tools help ensure that all requests are processed quickly and accurately. Additionally, users can access audit trails for compliance and record-keeping purposes.
-
How can airSlate SignNow benefit healthcare providers in managing Patient’s Request For Medical Payment?
By using airSlate SignNow, healthcare providers can enhance their efficiency in managing Patient’s Request For Medical Payment. The platform reduces administrative burdens, allowing staff to focus on patient care rather than paperwork. This leads to faster processing times and improved patient satisfaction.
-
Is airSlate SignNow secure for handling sensitive Patient’s Request For Medical Payment information?
Absolutely, airSlate SignNow prioritizes security and compliance, ensuring that all Patient’s Request For Medical Payment information is protected. The platform employs advanced encryption and adheres to industry standards for data protection. Users can trust that their sensitive information is safe throughout the entire process.
Get more for Patient s Request For Medical Payment
Find out other Patient s Request For Medical Payment
- How To eSign Virginia Business Operations Presentation
- How To eSign Hawaii Construction Word
- How Can I eSign Hawaii Construction Word
- How Can I eSign Hawaii Construction Word
- How Do I eSign Hawaii Construction Form
- How Can I eSign Hawaii Construction Form
- How To eSign Hawaii Construction Document
- Can I eSign Hawaii Construction Document
- How Do I eSign Hawaii Construction Form
- How To eSign Hawaii Construction Form
- How Do I eSign Hawaii Construction Form
- How To eSign Florida Doctors Form
- Help Me With eSign Hawaii Doctors Word
- How Can I eSign Hawaii Doctors Word
- Help Me With eSign New York Doctors PPT
- Can I eSign Hawaii Education PDF
- How To eSign Hawaii Education Document
- Can I eSign Hawaii Education Document
- How Can I eSign South Carolina Doctors PPT
- How Can I eSign Kansas Education Word