Wellcare Provider Payment Dispute Request Form


What is the Wellcare Provider Payment Dispute Request Form
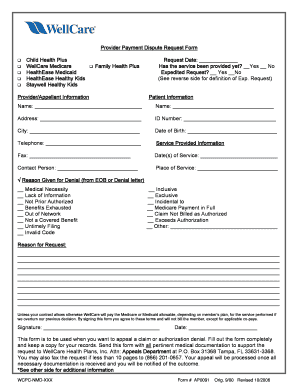
The Wellcare Provider Payment Dispute Request Form is a crucial document used by healthcare providers to formally contest payment decisions made by Wellcare. This form allows providers to outline the reasons for their dispute, ensuring that their concerns are documented and addressed. It is essential for maintaining transparent communication between Wellcare and its participating providers, facilitating a resolution process that is fair and efficient.
How to use the Wellcare Provider Payment Dispute Request Form
Using the Wellcare Provider Payment Dispute Request Form involves several steps. First, providers must accurately complete the form, providing all necessary details regarding the dispute. This includes information about the patient, the service rendered, and the specific payment issue being contested. Once filled out, the form should be submitted to Wellcare through the designated channels, which may include online submission or mailing it to the appropriate address. Ensuring that all information is accurate and complete will help expedite the review process.
Steps to complete the Wellcare Provider Payment Dispute Request Form
Completing the Wellcare Provider Payment Dispute Request Form requires careful attention to detail. Follow these steps:
- Gather all relevant information, including patient details and service dates.
- Clearly state the reason for the dispute, providing any supporting documentation.
- Fill out the form legibly, ensuring that all sections are completed.
- Review the form for accuracy before submission.
- Submit the form through the preferred method, keeping a copy for your records.
Legal use of the Wellcare Provider Payment Dispute Request Form
The Wellcare Provider Payment Dispute Request Form is legally recognized as a formal request for reconsideration of payment decisions. To ensure its legal validity, the form must be completed in accordance with Wellcare’s guidelines and submitted within the specified timeframe. Compliance with relevant regulations, such as the Health Insurance Portability and Accountability Act (HIPAA), is also essential to protect patient information during the dispute process.
Key elements of the Wellcare Provider Payment Dispute Request Form
Key elements of the Wellcare Provider Payment Dispute Request Form include:
- Provider identification information, including name and NPI number.
- Patient details, such as name and date of birth.
- Description of the service provided and the date it was rendered.
- Specific reasons for the dispute, including any relevant codes or references.
- Supporting documentation that substantiates the claim.
Form Submission Methods
Providers can submit the Wellcare Provider Payment Dispute Request Form through various methods. These typically include:
- Online submission via Wellcare's provider portal, which allows for immediate processing.
- Mailing the completed form to the designated address provided by Wellcare.
- In-person submission at Wellcare offices, if applicable.
Quick guide on how to complete wellcare provider payment dispute request form
Effortlessly Prepare Wellcare Provider Payment Dispute Request Form on Any Device
Digital document management has become widely adopted by businesses and individuals alike. It offers an ideal environmentally friendly substitute to traditional printed and signed paperwork, as you can obtain the correct form and securely save it online. airSlate SignNow equips you with all the resources necessary to create, edit, and electronically sign your documents swiftly without delays. Manage Wellcare Provider Payment Dispute Request Form on any device with airSlate SignNow's Android or iOS applications and streamline any document-related procedure today.
How to Edit and Electronically Sign Wellcare Provider Payment Dispute Request Form with Ease
- Find Wellcare Provider Payment Dispute Request Form and click Get Form to begin.
- Utilize the features we provide to complete your document.
- Emphasize important parts of the documents or conceal sensitive information using tools that airSlate SignNow offers specifically for this purpose.
- Create your electronic signature with the Sign tool, which takes mere seconds and carries the same legal validity as a traditional handwritten signature.
- Verify the details and click the Done button to save your changes.
- Choose how you wish to send your form, whether by email, text message (SMS), invitation link, or download it to your computer.
Eliminate the hassle of lost or misplaced documents, tedious form searching, or mistakes that necessitate printing new document copies. airSlate SignNow fulfills your document management needs in just a few clicks from your chosen device. Edit and electronically sign Wellcare Provider Payment Dispute Request Form and maintain excellent communication at every step of the form preparation process with airSlate SignNow.
Create this form in 5 minutes or less
Create this form in 5 minutes!
How to create an eSignature for the wellcare provider payment dispute request form
How to create an electronic signature for a PDF online
How to create an electronic signature for a PDF in Google Chrome
How to create an e-signature for signing PDFs in Gmail
How to create an e-signature right from your smartphone
How to create an e-signature for a PDF on iOS
How to create an e-signature for a PDF on Android
People also ask
-
What is a wellcare provider appeal form?
A wellcare provider appeal form is a document used by healthcare providers to appeal decisions made by WellCare regarding claims or services. This form allows providers to formally request a review of decisions that may have denied or underpaid their claims. Utilizing the wellcare provider appeal form ensures that your appeal process is standardized and compliant.
-
How can airSlate SignNow help with the wellcare provider appeal form?
airSlate SignNow streamlines the process of filling out and submitting the wellcare provider appeal form by providing a user-friendly interface for electronic signatures and document management. This saves time and reduces errors in submission, allowing providers to focus more on patient care rather than administrative tasks. With our solution, you can ensure that your appeals are processed efficiently.
-
What features does airSlate SignNow offer for managing the wellcare provider appeal form?
airSlate SignNow offers several features to facilitate managing the wellcare provider appeal form, including customizable templates, secure eSignature capabilities, and real-time tracking of document status. These features enhance collaboration within teams and ensure that all required documentation is complete before submission. This greatly enhances the appeal process for healthcare providers.
-
Is there a cost associated with using airSlate SignNow for the wellcare provider appeal form?
Yes, there is a cost associated with using airSlate SignNow for the wellcare provider appeal form, but our pricing plans are designed to be cost-effective and scalable. We offer different tiers to suit varying business needs, ensuring that you receive a service that fits your budget while maximizing your efficiency. Invest in airSlate SignNow to save time and resources in your appeal processes.
-
Can I integrate airSlate SignNow with other software while using the wellcare provider appeal form?
Absolutely! airSlate SignNow offers extensive integration capabilities with various software applications commonly used in healthcare and business. This includes electronic health record systems and practice management tools, allowing you to seamlessly manage your workflow when dealing with the wellcare provider appeal form. Integrations enhance your operational efficiency.
-
What are the benefits of using airSlate SignNow for the wellcare provider appeal form?
Using airSlate SignNow for the wellcare provider appeal form offers numerous benefits, including reducing paper usage, enhancing document security, and speeding up the submission process. Additionally, the electronic signing and tracking features increase accountability and transparency throughout the appeal process. These advantages lead to higher success rates in claim appeals.
-
How secure is the data when using airSlate SignNow for the wellcare provider appeal form?
Data security is a top priority at airSlate SignNow. When you use our platform for the wellcare provider appeal form, all sensitive information is protected with advanced encryption and secure storage solutions. Regular security audits and compliance with industry standards ensure that your data remains safe from unauthorized access.
Get more for Wellcare Provider Payment Dispute Request Form
- Ashgrove marketing 2016 calendar order form p
- New student tuition ampamp fee scheduleinternational school of form
- Ncsf recertification form
- Hanger plate carrier with form
- Glovalink form
- Lippert components warranty form
- Player and safeguarding welfare independent advice feedback key contacts the fa respect programme young players respect code of form
- Instruction for authors journal of the medical association of form
Find out other Wellcare Provider Payment Dispute Request Form
- How To Electronic signature Arkansas Construction Word
- How Do I Electronic signature Arkansas Construction Document
- Can I Electronic signature Delaware Construction PDF
- How Can I Electronic signature Ohio Business Operations Document
- How Do I Electronic signature Iowa Construction Document
- How Can I Electronic signature South Carolina Charity PDF
- How Can I Electronic signature Oklahoma Doctors Document
- How Can I Electronic signature Alabama Finance & Tax Accounting Document
- How To Electronic signature Delaware Government Document
- Help Me With Electronic signature Indiana Education PDF
- How To Electronic signature Connecticut Government Document
- How To Electronic signature Georgia Government PDF
- Can I Electronic signature Iowa Education Form
- How To Electronic signature Idaho Government Presentation
- Help Me With Electronic signature Hawaii Finance & Tax Accounting Document
- How Can I Electronic signature Indiana Government PDF
- How Can I Electronic signature Illinois Finance & Tax Accounting PPT
- How To Electronic signature Maine Government Document
- How To Electronic signature Louisiana Education Presentation
- How Can I Electronic signature Massachusetts Government PDF