Medical Necessity Certification 2005-2026


What is the Medical Necessity Certification
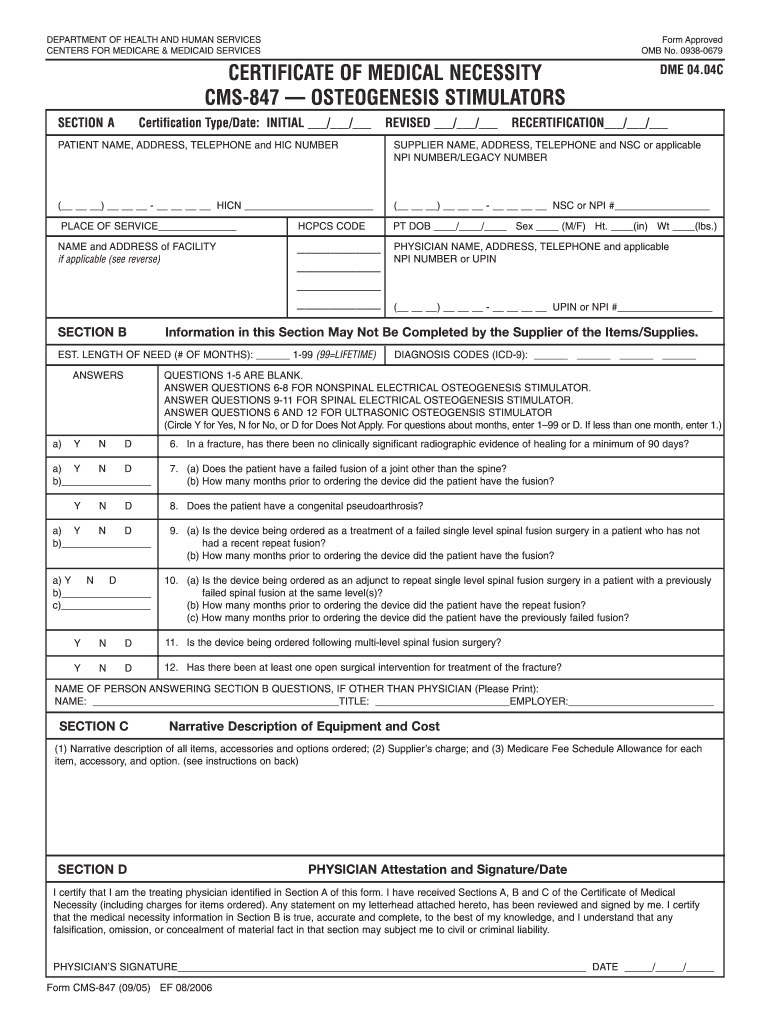
The certificate of medical necessity is a crucial document that verifies the medical need for specific services or equipment. It is often required by insurance companies, including Medicare, to justify the provision of medical supplies, durable medical equipment, or certain treatments. This certification ensures that the prescribed items are essential for the patient's health and well-being, aligning with the criteria set forth by healthcare providers and insurers.
How to Obtain the Medical Necessity Certification
To obtain a certificate of medical necessity, patients typically need to work closely with their healthcare providers. The process generally involves the following steps:
- Consult with a healthcare professional to discuss the necessity of the required medical equipment or service.
- Have the provider complete the medical necessity form, detailing the patient's condition and the justification for the requested items.
- Submit the completed form to the appropriate insurance company or Medicare for approval.
Steps to Complete the Medical Necessity Certification
Completing the certificate of medical necessity involves several key steps to ensure accuracy and compliance:
- Gather all necessary patient information, including medical history and current treatment plans.
- Fill out the form with precise details regarding the medical necessity, including specific diagnoses and prescribed items.
- Attach any required documentation, such as medical records or test results, to support the claim.
- Review the completed form for accuracy before submission to prevent delays in processing.
Legal Use of the Medical Necessity Certification
The legal use of the certificate of medical necessity is paramount for ensuring compliance with insurance requirements. This document must be completed accurately and submitted within specified time frames to avoid penalties. It serves as a legal record that can be referenced in case of disputes regarding coverage or reimbursement for medical services and equipment.
Key Elements of the Medical Necessity Certification
Several key elements must be included in the certificate of medical necessity to ensure its validity:
- Patient's full name and identifying information.
- Healthcare provider's information, including signature and credentials.
- A clear description of the medical condition necessitating the equipment or service.
- Specific details about the requested items, including codes and quantities.
- Justification for why these items are essential for the patient's treatment.
Form Submission Methods
Submitting the certificate of medical necessity can be done through various methods, depending on the requirements of the insurance provider:
- Online Submission: Many insurers allow electronic submissions through secure portals.
- Mail: Completed forms can be mailed to the insurance company, ensuring that all attachments are included.
- In-Person: Some patients may choose to deliver the forms directly to their insurance provider's office.
Quick guide on how to complete form cms 847
Discover the easiest method to complete and endorse your Medical Necessity Certification
Are you still spending time organizing your formal documents on paper instead of handling them online? airSlate SignNow provides a superior option to finalize and endorse your Medical Necessity Certification and other forms for public services. Our intelligent electronic signature platform equips you with all the tools necessary to manage paperwork efficiently and in accordance with official standards - powerful PDF editing, managing, safeguarding, signing, and sharing functionalities all accessible through a user-friendly interface.
There are just a few steps needed to complete and endorse your Medical Necessity Certification:
- Upload the editable template to the editor by clicking the Get Form button.
- Determine what information you need to include in your Medical Necessity Certification.
- Move between the fields using the Next button to ensure you don’t overlook anything.
- Utilize Text, Check, and Cross tools to fill in the sections with your information.
- Update the content with Text boxes or Images from the upper toolbar.
- Emphasize what is truly important or Blackout areas that are no longer relevant.
- Press Sign to generate a legally valid electronic signature using any method you choose.
- Add the Date next to your signature and complete your task with the Done button.
Store your completed Medical Necessity Certification in the Documents directory of your profile, download it, or export it to your chosen cloud storage. Our service also offers versatile file sharing options. There’s no need to print your forms when you need to submit them to the appropriate public office - handle it via email, fax, or by requesting USPS “snail mail” delivery from your account. Give it a try now!
Create this form in 5 minutes or less
FAQs
-
Do military members have to pay any fee for leave or fiancee forms?
NOOOOOOO. You are talking to a military romance scammer. I received an email from the US Army that directly answers your question that is pasted below please keep reading.I believe you are the victim of a military Romance Scam whereas the person you are talking to is a foreign national posing as an American Soldier claiming to be stationed overseas on a peacekeeping mission. That's the key to the scam they always claim to be on a peacekeeping mission.Part of their scam is saying that they have no access to their money that their mission is highly dangerous.If your boyfriend girlfriend/future husband/wife is asking you to do the following or has exhibited this behavior, it is a most likely a scam:Moves to private messaging site immediately after meeting you on Facebook or SnapChat or Instagram or some dating or social media site. Often times they delete the site you met them on right after they asked you to move to a more private messaging siteProfesses love to you very quickly & seems to quote poems and song lyrics along with using their own sort of broken language, as they profess their love and devotion quickly. They also showed concern for your health and love for your family.Promises marriage as soon as he/she gets to state for leave that they asked you to pay for.They Requests money (wire transfers) and Amazon, iTune ,Verizon, etc gift cards, for medicine, religious practices, and leaves to come home, internet access, complete job assignments, help sick friend, get him out of trouble, or anything that sounds fishy.The military does provide all the soldier needs including food medical Care and transportation for leave. Trust me, I lived it, you are probably being scammed. I am just trying to show you examples that you are most likely being connned.Below is an email response I received after I sent an inquiry to the US government when I discovered I was scammed. I received this wonderful response back with lots of useful links on how to find and report your scammer. And how to learn more about Romance Scams.Right now you can also copy the picture he gave you and do a google image search and you will hopefully see the pictures of the real person he is impersonating. this doesn't always work and take some digging. if you find the real person you can direct message them and alert them that their image is being used for scamming.Good Luck to you and I'm sorry this may be happening to you. please continue reading the government response I received below it's very informative. You have contacted an email that is monitored by the U.S. Army Criminal Investigation Command. Unfortunately, this is a common concern. We assure you there is never any reason to send money to anyone claiming to be a Soldier online. If you have only spoken with this person online, it is likely they are not a U.S. Soldier at all. If this is a suspected imposter social media profile, we urge you to report it to that platform as soon as possible. Please continue reading for more resources and answers to other frequently asked questions: How to report an imposter Facebook profile: Caution-https://www.facebook.com/help/16... < Caution-https://www.facebook.com/help/16... > Answers to frequently asked questions: - Soldiers and their loved ones are not charged money so that the Soldier can go on leave. - Soldiers are not charged money for secure communications or leave. - Soldiers do not need permission to get married. - Soldiers emails are in this format: john.doe.mil@mail.mil < Caution-mailto: john.doe.mil@mail.mil > anything ending in .us or .com is not an official email account. - Soldiers have medical insurance, which pays for their medical costs when treated at civilian health care facilities worldwide – family and friends do not need to pay their medical expenses. - Military aircraft are not used to transport Privately Owned Vehicles. - Army financial offices are not used to help Soldiers buy or sell items of any kind. - Soldiers deployed to Combat Zones do not need to solicit money from the public to feed or house themselves or their troops. - Deployed Soldiers do not find large unclaimed sums of money and need your help to get that money out of the country. Anyone who tells you one of the above-listed conditions/circumstances is true is likely posing as a Soldier and trying to steal money from you. We would urge you to immediately cease all contact with this individual. For more information on avoiding online scams and to report this crime, please see the following sites and articles: This article may help clarify some of the tricks social media scammers try to use to take advantage of people: Caution-https://www.army.mil/article/61432/< Caution-https://www.army.mil/article/61432/> CID advises vigilance against 'romance scams,' scammers impersonating Soldiers Caution-https://www.army.mil/article/180749 < Caution-https://www.army.mil/article/180749 > FBI Internet Crime Complaint Center: Caution-http://www.ic3.gov/default.aspx< Caution-http://www.ic3.gov/default.aspx> U.S. Army investigators warn public against romance scams: Caution-https://www.army.mil/article/130...< Caution-https://www.army.mil/article/130...> DOD warns troops, families to be cybercrime smart -Caution-http://www.army.mil/article/1450...< Caution-http://www.army.mil/article/1450...> Use caution with social networking Caution-https://www.army.mil/article/146...< Caution-https://www.army.mil/article/146...> Please see our frequently asked questions section under scams and legal issues. Caution-http://www.army.mil/faq/ < Caution-http://www.army.mil/faq/ > or visit Caution-http://www.cid.army.mil/ < Caution-http://www.cid.army.mil/ >. The challenge with most scams is determining if an individual is a legitimate member of the US Army. Based on the Privacy Act of 1974, we cannot provide this information. If concerned about a scam you may contact the Better Business Bureau (if it involves a solicitation for money), or local law enforcement. If you're involved in a Facebook or dating site scam, you are free to contact us direct; (571) 305-4056. If you have a social security number, you can find information about Soldiers online at Caution-https://www.dmdc.osd.mil/appj/sc... < Caution-https://www.dmdc.osd.mil/appj/sc... > . While this is a free search, it does not help you locate a retiree, but it can tell you if the Soldier is active duty or not. If more information is needed such as current duty station or location, you can contact the Commander Soldier's Records Data Center (SRDC) by phone or mail and they will help you locate individuals on active duty only, not retirees. There is a fee of $3.50 for businesses to use this service. The check or money order must be made out to the U.S. Treasury. It is not refundable. The address is: Commander Soldier's Records Data Center (SRDC) 8899 East 56th Street Indianapolis, IN 46249-5301 Phone: 1-866-771-6357 In addition, it is not possible to remove social networking site profiles without legitimate proof of identity theft or a scam. If you suspect fraud on this site, take a screenshot of any advances for money or impersonations and report the account on the social networking platform immediately. Please submit all information you have on this incident to Caution-www.ic3.gov < Caution-http://www.ic3.gov > (FBI website, Internet Criminal Complaint Center), immediately stop contact with the scammer (you are potentially providing them more information which can be used to scam you), and learn how to protect yourself against these scams at Caution-http://www.ftc.gov < Caution-http://www.ftc.gov > (Federal Trade Commission's website)
-
How can I fill out Google's intern host matching form to optimize my chances of receiving a match?
I was selected for a summer internship 2016.I tried to be very open while filling the preference form: I choose many products as my favorite products and I said I'm open about the team I want to join.I even was very open in the location and start date to get host matching interviews (I negotiated the start date in the interview until both me and my host were happy.) You could ask your recruiter to review your form (there are very cool and could help you a lot since they have a bigger experience).Do a search on the potential team.Before the interviews, try to find smart question that you are going to ask for the potential host (do a search on the team to find nice and deep questions to impress your host). Prepare well your resume.You are very likely not going to get algorithm/data structure questions like in the first round. It's going to be just some friendly chat if you are lucky. If your potential team is working on something like machine learning, expect that they are going to ask you questions about machine learning, courses related to machine learning you have and relevant experience (projects, internship). Of course you have to study that before the interview. Take as long time as you need if you feel rusty. It takes some time to get ready for the host matching (it's less than the technical interview) but it's worth it of course.
-
How do I fill out the form of DU CIC? I couldn't find the link to fill out the form.
Just register on the admission portal and during registration you will get an option for the entrance based course. Just register there. There is no separate form for DU CIC.
-
How do you know if you need to fill out a 1099 form?
Assuming that you are talking about 1099-MISC. Note that there are other 1099s.check this post - Form 1099 MISC Rules & RegulationsQuick answer - A Form 1099 MISC must be filed for each person to whom payment is made of:$600 or more for services performed for a trade or business by people not treated as employees;Rent or prizes and awards that are not for service ($600 or more) and royalties ($10 or more);any fishing boat proceeds,gross proceeds of $600, or more paid to an attorney during the year, orWithheld any federal income tax under the backup withholding rules regardless of the amount of the payment, etc.
-
How can I make it easier for users to fill out a form on mobile apps?
I’ll tell you a secret - you can thank me later for this.If you want to make the form-filling experience easy for a user - make sure that you have a great UI to offer.Everything boils down to UI at the end.Axonator is one of the best mobile apps to collect data since it offers powerful features bundled with a simple UI.The problem with most of the mobile form apps is that they are overloaded with features that aren’t really necessary.The same doesn’t hold true for Axonator. It has useful features but it is very unlikely that the user will feel overwhelmed in using them.So, if you are inclined towards having greater form completion rates for your survey or any data collection projects, then Axonator is the way to go.Apart from that, there are other features that make the data collection process faster like offline data collection, rich data capture - audio, video, images, QR code & barcode data capture, live location & time capture, and more!Check all the features here!You will be able to complete more surveys - because productivity will certainly shoot up.Since you aren’t using paper forms, errors will drop signNowly.The cost of the paper & print will be saved - your office expenses will drop dramatically.No repeat work. No data entry. Time & money saved yet again.Analytics will empower you to make strategic decisions and explore new revenue opportunities.The app is dirt-cheap & you don’t any training to use the app. They come in with a smooth UI. Forget using, even creating forms for your apps is easy on the platform. Just drag & drop - and it’s ready for use. Anyone can build an app under hours.
Create this form in 5 minutes!
How to create an eSignature for the form cms 847
How to generate an eSignature for the Form Cms 847 online
How to make an electronic signature for your Form Cms 847 in Google Chrome
How to generate an eSignature for putting it on the Form Cms 847 in Gmail
How to create an electronic signature for the Form Cms 847 straight from your smart phone
How to make an eSignature for the Form Cms 847 on iOS devices
How to create an electronic signature for the Form Cms 847 on Android
People also ask
-
What is Medical Necessity Certification and why is it important?
Medical Necessity Certification is a process that verifies the necessity of medical services or treatments for patients. This certification is crucial for ensuring that healthcare providers receive reimbursement from insurers, as it demonstrates that the services provided are essential for patient care.
-
How can airSlate SignNow help with obtaining Medical Necessity Certification?
airSlate SignNow simplifies the process of obtaining Medical Necessity Certification by allowing healthcare providers to quickly and securely send and eSign necessary documents. Our platform streamlines workflows, ensuring that certifications are processed efficiently and reducing delays in patient care.
-
What features does airSlate SignNow offer for Medical Necessity Certification?
airSlate SignNow offers features like customizable templates, real-time tracking, and secure electronic signatures that are perfect for Medical Necessity Certification. These tools enable healthcare providers to create, send, and manage certification documents seamlessly, ensuring compliance and efficiency.
-
Is airSlate SignNow compliant with healthcare regulations for Medical Necessity Certification?
Yes, airSlate SignNow is fully compliant with healthcare regulations such as HIPAA, making it a secure choice for handling Medical Necessity Certification documents. We prioritize data security to protect sensitive patient information throughout the certification process.
-
What are the pricing options for airSlate SignNow when handling Medical Necessity Certification?
airSlate SignNow offers flexible pricing plans that cater to businesses of all sizes, making it cost-effective for managing Medical Necessity Certification. You can choose from monthly or annual subscriptions based on your needs, with no hidden fees.
-
Can I integrate airSlate SignNow with other healthcare systems for Medical Necessity Certification?
Absolutely! airSlate SignNow seamlessly integrates with various healthcare management systems and EHR platforms, enhancing the process of Medical Necessity Certification. These integrations allow for better data flow and improved operational efficiency.
-
What benefits does airSlate SignNow provide for Medical Necessity Certification?
Using airSlate SignNow for Medical Necessity Certification offers numerous benefits, including faster turnaround times, reduced paperwork, and enhanced accuracy. It helps healthcare providers focus on patient care rather than administrative tasks.
Get more for Medical Necessity Certification
- Workers comp intake form
- Radiometer aqure user manual www3 hscni form
- Rma forms
- Acknowledgment of hearing notice court of appeals 9th circuit form
- Instructions application for raffle license this form is provided for bernards
- Promis eligible child demographic form intake form 1pdf
- Sports physical form 7 12 wilkes county health department
- 2014 financial aid application explo form
Find out other Medical Necessity Certification
- Sign North Carolina Construction Affidavit Of Heirship Later
- Sign Oregon Construction Emergency Contact Form Easy
- Sign Rhode Island Construction Business Plan Template Myself
- Sign Vermont Construction Rental Lease Agreement Safe
- Sign Utah Construction Cease And Desist Letter Computer
- Help Me With Sign Utah Construction Cease And Desist Letter
- Sign Wisconsin Construction Purchase Order Template Simple
- Sign Arkansas Doctors LLC Operating Agreement Free
- Sign California Doctors Lease Termination Letter Online
- Sign Iowa Doctors LLC Operating Agreement Online
- Sign Illinois Doctors Affidavit Of Heirship Secure
- Sign Maryland Doctors Quitclaim Deed Later
- How Can I Sign Maryland Doctors Quitclaim Deed
- Can I Sign Missouri Doctors Last Will And Testament
- Sign New Mexico Doctors Living Will Free
- Sign New York Doctors Executive Summary Template Mobile
- Sign New York Doctors Residential Lease Agreement Safe
- Sign New York Doctors Executive Summary Template Fast
- How Can I Sign New York Doctors Residential Lease Agreement
- Sign New York Doctors Purchase Order Template Online