PATIENT ACCESSAUTHORIZATION for USE or DISCLOSURE of PATIENT INFORMATION 2018-2026


Understanding the patient access authorization for use or disclosure of patient information
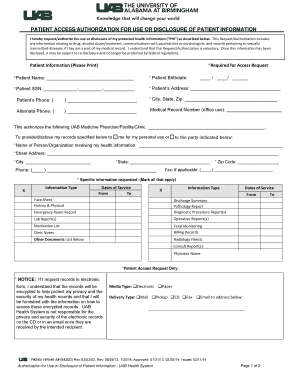
The patient access authorization for use or disclosure of patient information is a vital document that allows healthcare providers to share a patient's medical records with designated individuals or entities. This form is essential for maintaining the privacy and security of patient information while ensuring that necessary medical data can be accessed by authorized parties. Typically, this authorization is required under the Health Insurance Portability and Accountability Act (HIPAA), which sets standards for the protection of sensitive patient information.
The form outlines specific details, including the patient's name, the information to be disclosed, the purpose of the disclosure, and the duration of the authorization. By signing this document, patients give explicit permission for their healthcare providers to release their medical records to specified individuals or organizations, such as family members, other healthcare providers, or insurance companies.
Steps to complete the patient access authorization for use or disclosure of patient information
Completing the patient access authorization form involves several straightforward steps. First, ensure that you have the correct form, often available through your healthcare provider or their website. Next, fill in your personal information accurately, including your full name, date of birth, and contact information.
After providing your details, specify the information you wish to authorize for disclosure. This may include medical records, test results, or treatment plans. Clearly indicate the purpose of the disclosure, such as for insurance claims or transferring care to another provider. Finally, sign and date the form, and ensure that you provide any required witness signatures if applicable.
Legal use of the patient access authorization for use or disclosure of patient information
The legal use of the patient access authorization form is governed by federal and state laws, primarily HIPAA. This legislation ensures that patient information is disclosed only with the patient's consent and for legitimate purposes. Healthcare providers must retain this authorization for a specified period and can only disclose the information as outlined in the form.
It is crucial for patients to understand their rights regarding their medical information. They can revoke their authorization at any time, provided they do so in writing. This revocation must be communicated to the healthcare provider to prevent any further disclosures of their information.
Who issues the patient access authorization for use or disclosure of patient information
The patient access authorization form is typically issued by healthcare providers, such as hospitals, clinics, or private practices. Each provider may have their version of the form, tailored to comply with their specific policies and state regulations. Patients can request this form directly from their healthcare provider's office or access it through the provider's official website.
In some cases, third-party organizations, such as insurance companies or legal entities, may also provide a version of this form to facilitate the sharing of medical records related to claims or legal matters.
Key elements of the patient access authorization for use or disclosure of patient information
Several key elements must be included in the patient access authorization form to ensure its validity. These elements include:
- Patient Information: Full name, date of birth, and contact details.
- Recipient Information: Names and contact details of individuals or entities authorized to receive the information.
- Information to be Disclosed: Specific details about the medical records or information being shared.
- Purpose of Disclosure: A clear explanation of why the information is being shared.
- Expiration Date: The duration for which the authorization is valid.
- Signature: The patient's signature and date, confirming their consent.
How to obtain the patient access authorization for use or disclosure of patient information
To obtain the patient access authorization form, patients can start by contacting their healthcare provider's office. Most providers have the form readily available for patients upon request. Additionally, many healthcare facilities offer digital versions of the form on their websites, allowing patients to download and print it for completion.
If patients are unsure about the process or need assistance, they can consult with the administrative staff at their healthcare provider's office. Staff members are typically trained to guide patients through the authorization process and answer any questions regarding the information required or the implications of signing the form.
Quick guide on how to complete patient accessauthorization for use or disclosure of patient information
Effortlessly Prepare PATIENT ACCESSAUTHORIZATION FOR USE OR DISCLOSURE OF PATIENT INFORMATION on Any Device
Managing documents online has become increasingly popular among companies and individuals. It offers an ideal environmentally friendly alternative to traditional printed and signed paperwork, allowing you to access the necessary form and securely store it online. airSlate SignNow provides all the resources you require to create, modify, and electronically sign your documents promptly without delays. Handle PATIENT ACCESSAUTHORIZATION FOR USE OR DISCLOSURE OF PATIENT INFORMATION on any platform using airSlate SignNow's Android or iOS applications and simplify any document-related task today.
How to Modify and Electronically Sign PATIENT ACCESSAUTHORIZATION FOR USE OR DISCLOSURE OF PATIENT INFORMATION with Ease
- Locate PATIENT ACCESSAUTHORIZATION FOR USE OR DISCLOSURE OF PATIENT INFORMATION and click on Get Form to begin.
- Utilize the tools we offer to fill out your document.
- Emphasize important sections of the documents or redact sensitive information with tools specifically provided by airSlate SignNow.
- Create your electronic signature using the Sign feature, which takes just seconds and carries the same legal validity as a conventional wet ink signature.
- Review all the information carefully and then click on the Done button to save your updates.
- Select your preferred method to send your form, whether by email, SMS, invitation link, or download it to your computer.
Eliminate the hassle of lost or misplaced documents, tedious form searches, or errors that require reprinting. airSlate SignNow meets your document management needs in just a few clicks from your chosen device. Edit and electronically sign PATIENT ACCESSAUTHORIZATION FOR USE OR DISCLOSURE OF PATIENT INFORMATION and ensure excellent communication throughout your form preparation process with airSlate SignNow.
Create this form in 5 minutes or less
Find and fill out the correct patient accessauthorization for use or disclosure of patient information
Create this form in 5 minutes!
How to create an eSignature for the patient accessauthorization for use or disclosure of patient information
The way to create an electronic signature for your PDF file in the online mode
The way to create an electronic signature for your PDF file in Chrome
How to make an eSignature for putting it on PDFs in Gmail
The best way to make an electronic signature right from your smartphone
The best way to create an electronic signature for a PDF file on iOS devices
The best way to make an electronic signature for a PDF on Android
People also ask
-
What is patient access authorization for use or disclosure of patient information?
PATIENT ACCESSAUTHORIZATION FOR USE OR DISCLOSURE OF PATIENT INFORMATION is a legal document that allows healthcare providers to share a patient’s medical records with authorized individuals or entities. This authorization ensures compliance with privacy laws, allowing patients to control who has access to their sensitive health information.
-
How does airSlate SignNow simplify the process of obtaining patient access authorization?
airSlate SignNow streamlines the process of obtaining PATIENT ACCESSAUTHORIZATION FOR USE OR DISCLOSURE OF PATIENT INFORMATION by providing customizable templates and an easy-to-use interface. With our solution, healthcare providers can quickly create, send, and track authorization forms, making it easier for patients to grant permission for their information to be shared.
-
Are there any costs associated with using airSlate SignNow for patient access authorization?
Yes, airSlate SignNow offers a variety of pricing plans tailored to different needs, including options specifically for healthcare organizations needing to manage PATIENT ACCESSAUTHORIZATION FOR USE OR DISCLOSURE OF PATIENT INFORMATION. Our plans are designed to be cost-effective, ensuring you get the best value while maintaining compliance and enhancing patient engagement.
-
What features does airSlate SignNow offer for managing patient information authorization?
airSlate SignNow includes features such as customizable templates, secure eSignature capabilities, and automated reminders for PATIENT ACCESSAUTHORIZATION FOR USE OR DISCLOSURE OF PATIENT INFORMATION. These features help healthcare providers efficiently manage authorizations while ensuring that patient data remains secure and compliant with regulations.
-
Can I integrate airSlate SignNow with other healthcare software?
Yes, airSlate SignNow can be integrated with various healthcare systems and software platforms, enhancing your workflow for managing PATIENT ACCESSAUTHORIZATION FOR USE OR DISCLOSURE OF PATIENT INFORMATION. This integration allows for seamless data transfer and improved efficiency, ensuring that your patient information management is streamlined.
-
What benefits does airSlate SignNow provide for patient access authorization?
Using airSlate SignNow for PATIENT ACCESSAUTHORIZATION FOR USE OR DISCLOSURE OF PATIENT INFORMATION offers numerous benefits, including improved efficiency, enhanced security, and better compliance with healthcare regulations. Our platform ensures that obtaining and managing patient authorizations is straightforward, reducing administrative burdens and fostering better patient-provider relationships.
-
Is airSlate SignNow compliant with HIPAA regulations?
Yes, airSlate SignNow is fully compliant with HIPAA regulations, ensuring that all PATIENT ACCESSAUTHORIZATION FOR USE OR DISCLOSURE OF PATIENT INFORMATION is handled securely and confidentially. We prioritize the protection of patient data, making it a trusted solution for healthcare organizations.
Get more for PATIENT ACCESSAUTHORIZATION FOR USE OR DISCLOSURE OF PATIENT INFORMATION
- Form i 918 supplement b u nonimmigrant status certification
- Alaska employer registration form for daycare services
- Driver abstract consent this form is used by a person to grant the release of their driver abstract to a person that is known
- Va form 21 0960j 1 kidney conditions nephrology disability benefits questionnaire
- Va form 26 4555c veteranservicemembers supplemental application for
- Form a29 labour relations act 1995 application regarding union s duty of fair representation before the ontario labour
- 2018 m4 corporation franchise tax return corporation franchise tax return 2018 form
- Imm5644 form
Find out other PATIENT ACCESSAUTHORIZATION FOR USE OR DISCLOSURE OF PATIENT INFORMATION
- Help Me With Electronic signature West Virginia Non-Profit Business Plan Template
- Electronic signature Nebraska Legal Living Will Simple
- Electronic signature Nevada Legal Contract Safe
- How Can I Electronic signature Nevada Legal Operating Agreement
- How Do I Electronic signature New Hampshire Legal LLC Operating Agreement
- How Can I Electronic signature New Mexico Legal Forbearance Agreement
- Electronic signature New Jersey Legal Residential Lease Agreement Fast
- How To Electronic signature New York Legal Lease Agreement
- How Can I Electronic signature New York Legal Stock Certificate
- Electronic signature North Carolina Legal Quitclaim Deed Secure
- How Can I Electronic signature North Carolina Legal Permission Slip
- Electronic signature Legal PDF North Dakota Online
- Electronic signature North Carolina Life Sciences Stock Certificate Fast
- Help Me With Electronic signature North Dakota Legal Warranty Deed
- Electronic signature North Dakota Legal Cease And Desist Letter Online
- Electronic signature North Dakota Legal Cease And Desist Letter Free
- Electronic signature Delaware Orthodontists Permission Slip Free
- How Do I Electronic signature Hawaii Orthodontists Lease Agreement Form
- Electronic signature North Dakota Life Sciences Business Plan Template Now
- Electronic signature Oklahoma Legal Bill Of Lading Fast