Pharmacy Prior Authorization Form Connecticut Medical


What is the Connecticut Medicaid Prior Authorization Form?
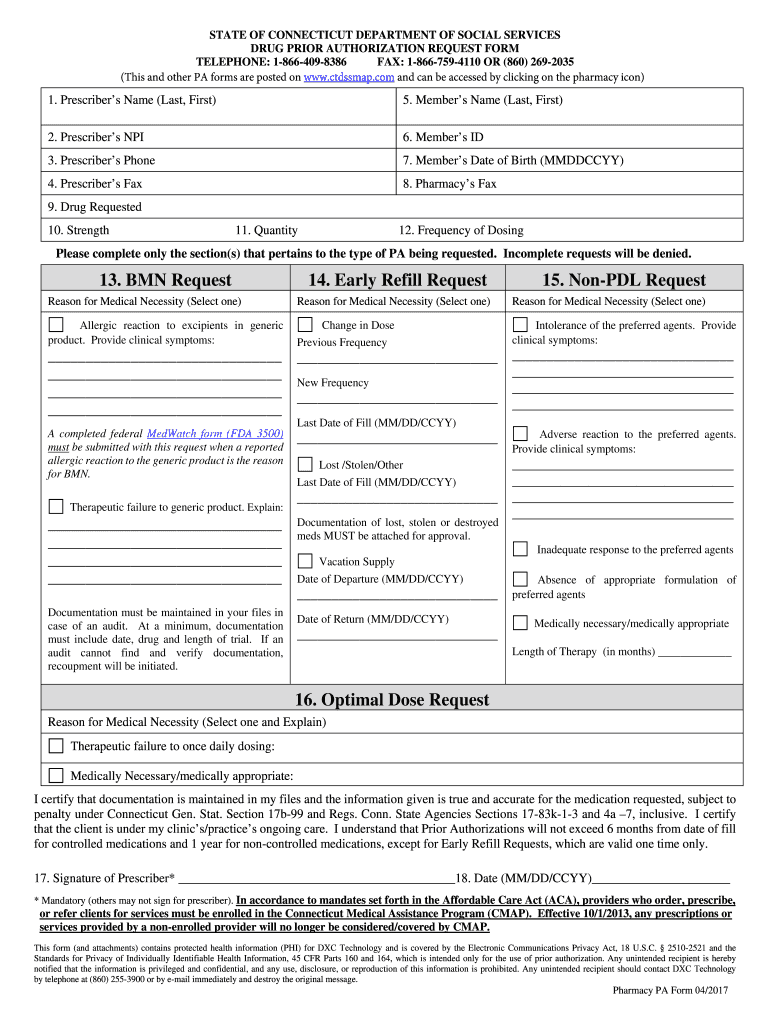
The Connecticut Medicaid prior authorization form is a document required for certain medical services and medications under the Connecticut Medicaid program. This form is essential for healthcare providers to obtain approval before administering specific treatments or prescribing medications that may not be automatically covered by Medicaid. The prior authorization process helps ensure that the prescribed services or medications are medically necessary and appropriate for the patient’s condition.
Steps to Complete the Connecticut Medicaid Prior Authorization Form
Completing the Connecticut Medicaid prior authorization form involves several important steps to ensure accuracy and compliance. Here is a structured approach to filling out the form:
- Gather Patient Information: Collect all necessary patient details, including name, date of birth, and Medicaid identification number.
- Provide Provider Information: Include the healthcare provider's name, contact information, and NPI (National Provider Identifier) number.
- Detail the Requested Service or Medication: Clearly specify the service or medication requiring prior authorization, including dosage and frequency.
- Document Medical Necessity: Provide clinical information and rationale supporting the need for the requested service or medication.
- Review and Sign: Ensure all information is accurate, then sign and date the form before submission.
How to Obtain the Connecticut Medicaid Prior Authorization Form
The Connecticut Medicaid prior authorization form can be obtained through various channels. Healthcare providers can access the form online via the Connecticut Department of Social Services website or request it directly from Medicaid offices. Additionally, many healthcare facilities maintain copies of the form for their staff to use when submitting prior authorization requests.
Legal Use of the Connecticut Medicaid Prior Authorization Form
The Connecticut Medicaid prior authorization form is legally binding once completed and signed. It must adhere to specific regulations set forth by Medicaid to ensure that the authorization process is valid. Compliance with these regulations includes providing accurate patient information, documenting medical necessity, and obtaining the appropriate signatures. Failure to comply with these legal requirements may result in delays or denials of authorization requests.
Key Elements of the Connecticut Medicaid Prior Authorization Form
Understanding the key elements of the Connecticut Medicaid prior authorization form is crucial for successful completion. Important components include:
- Patient Information: Essential details about the patient.
- Provider Information: Identification of the healthcare provider requesting authorization.
- Requested Service or Medication: Clear description of what is being requested.
- Clinical Justification: Evidence supporting the need for the service or medication.
- Signatures: Required signatures from both the provider and the patient, if applicable.
Form Submission Methods for the Connecticut Medicaid Prior Authorization Form
Submitting the Connecticut Medicaid prior authorization form can be done through various methods, ensuring flexibility for healthcare providers. Options include:
- Online Submission: Many providers can submit the form electronically through the Connecticut Medicaid portal.
- Mail: The completed form can be mailed to the appropriate Medicaid office.
- In-Person: Providers may also submit the form in person at designated Medicaid locations.
Quick guide on how to complete pharmacy prior authorization form connecticut medical
Complete Pharmacy Prior Authorization Form Connecticut Medical effortlessly on any gadget
Digital document administration has gained traction among businesses and individuals. It offers an excellent eco-friendly substitute for traditional printed and signed documents, allowing you to find the correct template and securely store it online. airSlate SignNow equips you with all the resources required to create, modify, and eSign your documents swiftly without hindrances. Manage Pharmacy Prior Authorization Form Connecticut Medical on any gadget with airSlate SignNow applications for Android or iOS and streamline any document-related task today.
How to modify and eSign Pharmacy Prior Authorization Form Connecticut Medical effortlessly
- Find Pharmacy Prior Authorization Form Connecticut Medical and click on Get Form to begin.
- Utilize the features we provide to finish your form.
- Emphasize pertinent sections of the documents or obscure sensitive information with tools that airSlate SignNow supplies specifically for that purpose.
- Create your eSignature using the Sign tool, which takes just seconds and carries the same legal significance as a conventional wet ink signature.
- Review the details and click on the Done button to save your modifications.
- Select your preferred method to send your form, via email, text message (SMS), invitation link, or download it to your computer.
Eliminate concerns about lost or misplaced files, tedious form searching, or errors that require printing additional document copies. airSlate SignNow fulfills all your document management needs in just a few clicks from any gadget of your choice. Modify and eSign Pharmacy Prior Authorization Form Connecticut Medical and guarantee excellent communication at any stage of your form development process with airSlate SignNow.
Create this form in 5 minutes or less
Create this form in 5 minutes!
How to create an eSignature for the pharmacy prior authorization form connecticut medical
How to generate an eSignature for a PDF file online
How to generate an eSignature for a PDF file in Google Chrome
How to create an electronic signature for signing PDFs in Gmail
How to make an eSignature right from your mobile device
The best way to create an eSignature for a PDF file on iOS
How to make an eSignature for a PDF on Android devices
People also ask
-
What is a CT Medicaid prior authorization form?
A CT Medicaid prior authorization form is a document required for some medical services or prescriptions to ensure coverage under Connecticut's Medicaid program. This form typically must be completed by a healthcare provider and submitted to the Medicaid program for approval before the service is rendered.
-
How can airSlate SignNow help with CT Medicaid prior authorization forms?
airSlate SignNow simplifies the process of sending and electronically signing CT Medicaid prior authorization forms. Our platform allows healthcare providers to efficiently prepare, sign, and submit these forms, reducing delays and improving overall workflow.
-
Is there a cost associated with using airSlate SignNow for CT Medicaid prior authorization forms?
Yes, airSlate SignNow offers a cost-effective solution for managing CT Medicaid prior authorization forms. Our pricing plans are designed to fit different needs, and we provide a free trial to help you explore our features and determine the best package for your organization.
-
What features does airSlate SignNow offer for handling CT Medicaid prior authorization forms?
airSlate SignNow includes features like template creation, easy document sharing, and real-time signing notifications, making it ideal for managing CT Medicaid prior authorization forms. Additionally, users can track the status of their submissions, ensuring nothing falls through the cracks.
-
Can airSlate SignNow integrate with other software for processing CT Medicaid prior authorization forms?
Absolutely! airSlate SignNow integrates seamlessly with various healthcare management systems and electronic health records, facilitating the smooth handling of CT Medicaid prior authorization forms. These integrations ensure that your workflow is efficient and that you can access all necessary information in one place.
-
Are there any benefits to using airSlate SignNow for CT Medicaid prior authorization forms?
Using airSlate SignNow for CT Medicaid prior authorization forms provides a range of benefits including quicker turnaround times, reduced paperwork, and improved compliance. Our eSigning and automation features minimize errors and streamline the entire authorization process.
-
How secure is the airSlate SignNow platform for CT Medicaid prior authorization forms?
airSlate SignNow prioritizes the security of user data and documents. When handling CT Medicaid prior authorization forms, we adhere to industry-standard security protocols, including encryption and access controls, to protect sensitive information.
Get more for Pharmacy Prior Authorization Form Connecticut Medical
Find out other Pharmacy Prior Authorization Form Connecticut Medical
- Electronic signature Michigan Banking Affidavit Of Heirship Fast
- Electronic signature Arizona Business Operations Job Offer Free
- Electronic signature Nevada Banking NDA Online
- Electronic signature Nebraska Banking Confidentiality Agreement Myself
- Electronic signature Alaska Car Dealer Resignation Letter Myself
- Electronic signature Alaska Car Dealer NDA Mobile
- How Can I Electronic signature Arizona Car Dealer Agreement
- Electronic signature California Business Operations Promissory Note Template Fast
- How Do I Electronic signature Arkansas Car Dealer Claim
- Electronic signature Colorado Car Dealer Arbitration Agreement Mobile
- Electronic signature California Car Dealer Rental Lease Agreement Fast
- Electronic signature Connecticut Car Dealer Lease Agreement Now
- Electronic signature Connecticut Car Dealer Warranty Deed Computer
- Electronic signature New Mexico Banking Job Offer Online
- How Can I Electronic signature Delaware Car Dealer Purchase Order Template
- How To Electronic signature Delaware Car Dealer Lease Template
- Electronic signature North Carolina Banking Claim Secure
- Electronic signature North Carolina Banking Separation Agreement Online
- How Can I Electronic signature Iowa Car Dealer Promissory Note Template
- Electronic signature Iowa Car Dealer Limited Power Of Attorney Myself