Authorization to Use or Disclose Health Info Form


What is the authorization to use or disclose health info?
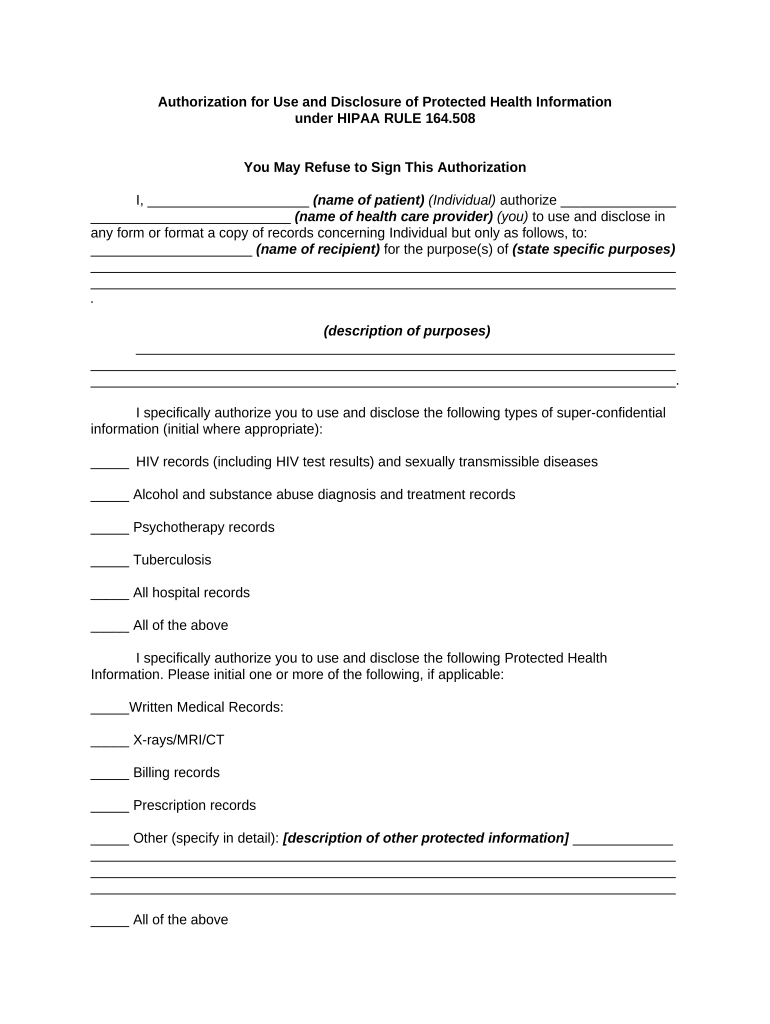
The authorization to use or disclose health information is a legal document that allows healthcare providers and organizations to share a patient's medical records and other health-related information with third parties. This authorization is crucial for ensuring that sensitive health data is handled appropriately and in compliance with privacy laws such as HIPAA. It outlines what information can be shared, with whom, and for what purpose, ensuring that patients have control over their personal health data.
How to use the authorization to use or disclose health info
Using the authorization to use or disclose health information involves several key steps. First, the patient must complete the authorization form, providing necessary details such as their name, the specific information to be shared, and the recipient's information. Next, the patient must sign and date the form to validate it. Once completed, the form can be submitted to the healthcare provider or organization, which will then process the request according to the outlined terms. It is important to keep a copy of the signed authorization for personal records.
Steps to complete the authorization to use or disclose health info
Completing the authorization to use or disclose health information typically involves the following steps:
- Obtain the authorization form from your healthcare provider or organization.
- Fill out your personal information, including your name, address, and date of birth.
- Specify the information you wish to authorize for disclosure.
- Indicate the recipient of the information and their contact details.
- State the purpose of the disclosure, such as for treatment or insurance purposes.
- Sign and date the form to validate your authorization.
- Submit the completed form to the appropriate healthcare provider.
Legal use of the authorization to use or disclose health info
The legal use of the authorization to use or disclose health information is governed by federal and state laws, primarily the Health Insurance Portability and Accountability Act (HIPAA). This legislation ensures that patient information is protected and can only be shared with explicit consent. The authorization must meet specific criteria to be considered valid, including being clear, specific, and not overly broad. Healthcare entities must also ensure that they comply with any state-specific regulations that may impose additional requirements.
Key elements of the authorization to use or disclose health info
Key elements of the authorization to use or disclose health information include:
- Patient Information: Full name, address, and date of birth of the patient.
- Information to be Disclosed: Specific details about the health information being shared.
- Recipient Information: Name and contact details of the individual or organization receiving the information.
- Purpose of Disclosure: Clear statement of why the information is being shared.
- Expiration Date: Indication of when the authorization will expire or if it is valid indefinitely.
- Signature: The patient’s signature and date to confirm consent.
Disclosure requirements
Disclosure requirements for the authorization to use or disclose health information vary based on the nature of the request and the laws governing health information privacy. Generally, the authorization must specify what information is being disclosed, to whom it is being disclosed, and for what purpose. It is essential that the healthcare provider ensures that the disclosure is compliant with HIPAA regulations and any relevant state laws. Additionally, patients should be informed about their rights regarding their health information, including the right to revoke the authorization at any time.
Quick guide on how to complete authorization to use or disclose health info
Effortlessly Prepare Authorization To Use Or Disclose Health Info on Any Device
Digital document management has gained popularity among businesses and individuals alike. It serves as a perfect eco-friendly alternative to conventional printed and signed papers, allowing you to obtain the necessary form and securely store it online. airSlate SignNow provides you with all the resources required to create, modify, and electronically sign your documents quickly without delays. Manage Authorization To Use Or Disclose Health Info on any platform using the airSlate SignNow Android or iOS applications and simplify any document-related process today.
The Easiest Way to Modify and Electronically Sign Authorization To Use Or Disclose Health Info Seamlessly
- Find Authorization To Use Or Disclose Health Info and click Get Form to begin.
- Use the tools we provide to fill out your document.
- Mark important sections of the documents or redact sensitive information using the tools that airSlate SignNow offers specifically for that purpose.
- Create your signature with the Sign tool, which takes only seconds and holds the same legal validity as a traditional ink signature.
- Review all details and click the Done button to save your modifications.
- Choose how you wish to send your form—via email, SMS, or invitation link—or download it to your PC.
Leave behind concerns about lost or misplaced documents, exhausting form searching, or errors that necessitate printing new copies. airSlate SignNow fulfills your document management needs with just a few clicks from any device of your choosing. Edit and electronically sign Authorization To Use Or Disclose Health Info while ensuring clear communication at every stage of the form preparation process with airSlate SignNow.
Create this form in 5 minutes or less
Create this form in 5 minutes!
People also ask
-
What is authorization health information?
Authorization health information refers to the documentation required for healthcare providers to obtain consent from patients for sharing their health data. This process is essential for maintaining patient privacy and ensuring compliance with regulations. airSlate SignNow simplifies this process by providing a seamless eSignature solution for handling authorization health information.
-
How does airSlate SignNow help with managing authorization health information?
airSlate SignNow streamlines the management of authorization health information by allowing healthcare organizations to send, sign, and store documents electronically. With its easy-to-use interface, you can quickly obtain patient signatures on authorization forms, reducing paperwork and improving efficiency in your practice. This ensures that you can manage authorization health information effectively.
-
Is there a cost associated with using airSlate SignNow for authorization health information?
Yes, airSlate SignNow offers various pricing plans tailored to different business sizes and needs, making it a cost-effective solution for managing authorization health information. You can choose from different subscription tiers based on your requirements. Our transparent pricing ensures you only pay for the features you utilize.
-
What features does airSlate SignNow provide for handling authorization health information?
airSlate SignNow offers intuitive features such as customizable templates, secure cloud storage, and real-time tracking for routing authorization health information. Additionally, its robust security measures protect sensitive data, ensuring compliance with healthcare regulations. These features enhance the overall efficiency of managing authorization health information.
-
Can airSlate SignNow integrate with other health software for authorization health information?
Yes, airSlate SignNow integrates seamlessly with various healthcare software systems, enabling you to manage authorization health information within your existing workflows. Our integrations facilitate data sharing and streamline processes across platforms. This ensures you can maintain operational efficiency while managing essential patient consent documentation.
-
What benefits does airSlate SignNow offer for healthcare providers managing authorization health information?
airSlate SignNow provides healthcare providers with benefits like reduced turnaround time for document processing and improved patient engagement when managing authorization health information. The platform automates the collection of signatures, minimizing delays in treatment and enhancing patient satisfaction. This leads to better overall patient care and operational efficiency.
-
How secure is airSlate SignNow when handling authorization health information?
Security is a top priority at airSlate SignNow, especially for handling authorization health information. Our platform employs advanced encryption and secure data handling practices to protect sensitive health data. Compliance with industry regulations ensures that your authorization health information stays confidential and secure throughout the signing process.
Get more for Authorization To Use Or Disclose Health Info
Find out other Authorization To Use Or Disclose Health Info
- How To eSign Wisconsin Education PDF
- Help Me With eSign Nebraska Finance & Tax Accounting PDF
- How To eSign North Carolina Finance & Tax Accounting Presentation
- How To eSign North Dakota Finance & Tax Accounting Presentation
- Help Me With eSign Alabama Healthcare / Medical PDF
- How To eSign Hawaii Government Word
- Can I eSign Hawaii Government Word
- How To eSign Hawaii Government Document
- How To eSign Hawaii Government Document
- How Can I eSign Hawaii Government Document
- Can I eSign Hawaii Government Document
- How Can I eSign Hawaii Government Document
- How To eSign Hawaii Government Document
- How To eSign Hawaii Government Form
- How Can I eSign Hawaii Government Form
- Help Me With eSign Hawaii Healthcare / Medical PDF
- How To eSign Arizona High Tech Document
- How Can I eSign Illinois Healthcare / Medical Presentation
- Can I eSign Hawaii High Tech Document
- How Can I eSign Hawaii High Tech Document