
Fill and Sign the Bank of Ireland Transaction Dispute Form 50526690
Valuable assistance on preparing your ‘Bank Of Ireland Transaction Dispute Form 50526690’ online
Are you fed up with the inconvenience of handling paperwork? Look no further than airSlate SignNow, the leading electronic signature solution for individuals and small to medium-sized businesses. Bid farewell to the tedious routine of printing and scanning documents. With airSlate SignNow, you can effortlessly fill out and sign documents online. Take advantage of the comprehensive features included in this user-friendly and cost-effective platform and transform your method of managing paperwork. Whether you need to sign documents or gather electronic signatures, airSlate SignNow manages everything effortlessly, with just a few clicks.
Adhere to this step-by-step guide:
- Access your account or register for a complimentary trial with our service.
- Click +Create to upload a file from your device, cloud storage, or our template library.
- Open your ‘Bank Of Ireland Transaction Dispute Form 50526690’ in the editor.
- Click Me (Fill Out Now) to finish the document on your end.
- Add and designate fillable fields for others (if necessary).
- Proceed with the Send Invite settings to solicit eSignatures from others.
- Download, print your version, or convert it into a reusable template.
No need to worry if you have to collaborate with your colleagues on your Bank Of Ireland Transaction Dispute Form 50526690 or send it for notarization—our platform provides everything you require to accomplish these tasks. Create an account with airSlate SignNow today and enhance your document management to a new level!
FAQs
-
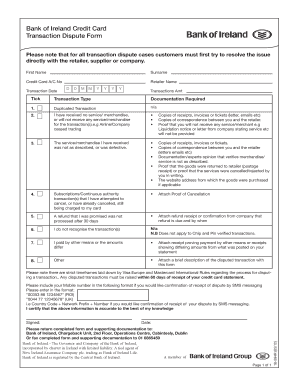
What is the Bank Of Ireland Transaction Dispute Form?
The Bank Of Ireland Transaction Dispute Form is a document designed for customers to formally dispute transactions on their accounts. By using this form, you can provide essential information regarding the disputed transaction, facilitating a smoother resolution process with your bank.
-
How do I access the Bank Of Ireland Transaction Dispute Form?
You can easily access the Bank Of Ireland Transaction Dispute Form through your Bank of Ireland online banking portal or by visiting their official website. Additionally, airSlate SignNow can help you eSign and send this form seamlessly, ensuring a quick submission.
-
Can I edit the Bank Of Ireland Transaction Dispute Form?
Yes, you can edit the Bank Of Ireland Transaction Dispute Form before submitting it. Using airSlate SignNow, you can customize the form with your details and any supporting information, making it a convenient tool for managing your disputes.
-
What features does airSlate SignNow offer for the Bank Of Ireland Transaction Dispute Form?
airSlate SignNow provides features that allow users to easily fill, eSign, and share the Bank Of Ireland Transaction Dispute Form. With intuitive tools for document management and tracking, you can ensure all necessary steps are followed for a successful dispute.
-
Is there a cost associated with using the Bank Of Ireland Transaction Dispute Form through airSlate SignNow?
While the Bank Of Ireland Transaction Dispute Form is free to access, using airSlate SignNow may involve subscription fees depending on the plan you choose. However, the cost is often justified by the efficiency and ease it brings to the document signing process.
-
What are the benefits of using airSlate SignNow for the Bank Of Ireland Transaction Dispute Form?
Using airSlate SignNow for the Bank Of Ireland Transaction Dispute Form streamlines the process of filling out and submitting your dispute. The platform’s user-friendly interface and secure eSigning capabilities enhance the overall experience and improve response times from the bank.
-
Does airSlate SignNow integrate with other tools for handling the Bank Of Ireland Transaction Dispute Form?
Yes, airSlate SignNow integrates with various tools and platforms, allowing you to manage the Bank Of Ireland Transaction Dispute Form alongside your other business documents. This integration ensures a cohesive workflow and enhances productivity when dealing with financial disputes.
Find out other bank of ireland transaction dispute form 50526690
- Close deals faster
- Improve productivity
- Delight customers
- Increase revenue
- Save time & money
- Reduce payment cycles
