
Fill and Sign the Health Insurance Application for Extended Family Planning Benefits Form
Valuable advice on preparing your ‘Health Insurance Application For Extended Family Planning Benefits ’ online
Feeling overwhelmed by the burden of paperwork? Look no further than airSlate SignNow, the premier electronic signature platform for both individuals and small to medium-sized businesses. Eliminate the tedious routine of printing and scanning documents. With airSlate SignNow, you can effortlessly complete and sign documents digitally. Take advantage of the powerful features integrated into this user-friendly and cost-effective platform and transform your document management strategy. Whether you need to sign forms or collect eSignatures, airSlate SignNow simplifies the process with just a few clicks.
Follow this step-by-step guide:
- Access your account or register for a complimentary trial with our service.
- Select +Create to upload a file from your device, cloud storage, or our form library.
- Open your ‘Health Insurance Application For Extended Family Planning Benefits ’ in the editor.
- Click Me (Fill Out Now) to complete the document on your end.
- Add and designate fillable fields for others (if necessary).
- Proceed with the Send Invite settings to solicit eSignatures from others.
- Save, print your version, or convert it into a reusable template.
No need to worry if you want to collaborate with your colleagues on your Health Insurance Application For Extended Family Planning Benefits or send it for notarization—our solution has everything you require to get the job done. Sign up with airSlate SignNow today and elevate your document management to the next level!
FAQs
-
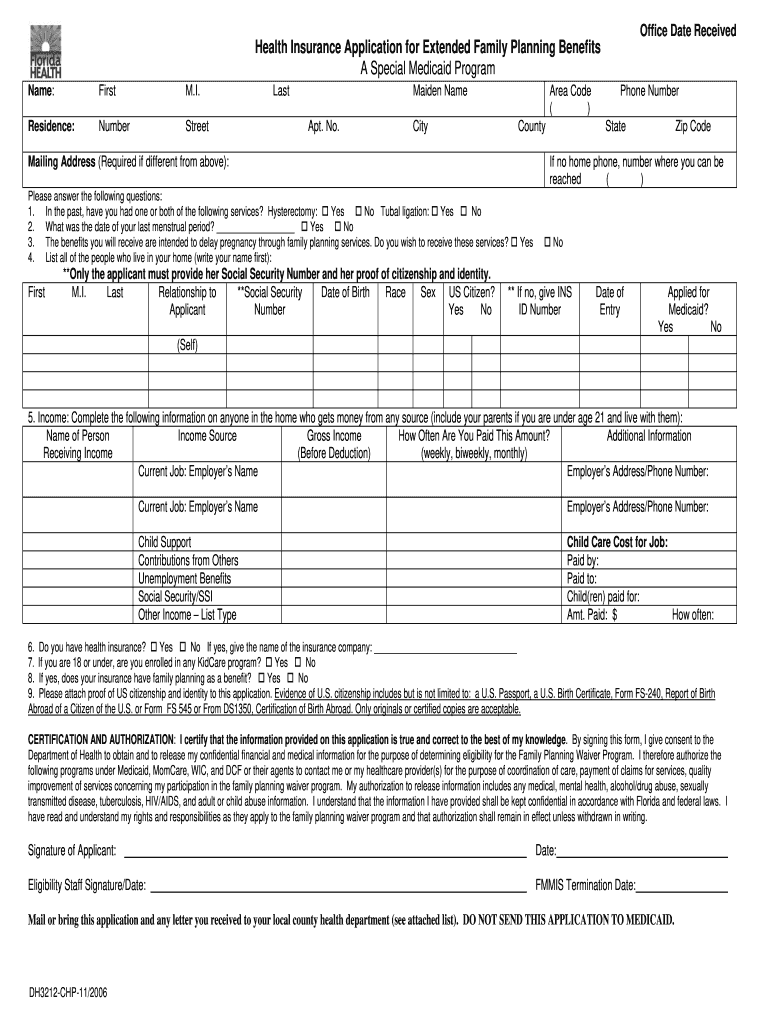
What is the Health Insurance Application For Extended Family Planning Benefits?
The Health Insurance Application For Extended Family Planning Benefits is a comprehensive form designed to help families access essential health insurance coverage for extended family planning services. This application ensures that all necessary information is collected efficiently, streamlining the process for families seeking these important benefits.
-
How can airSlate SignNow assist with the Health Insurance Application For Extended Family Planning Benefits?
airSlate SignNow provides a user-friendly platform that allows you to easily send and eSign the Health Insurance Application For Extended Family Planning Benefits. With its intuitive interface, you can manage all your documents securely and efficiently, ensuring that your application is submitted promptly.
-
What are the key features of airSlate SignNow for handling health insurance applications?
Key features of airSlate SignNow include customizable templates, secure eSigning, and real-time collaboration tools, all of which enhance the process of submitting a Health Insurance Application For Extended Family Planning Benefits. These features help reduce paperwork errors and speed up approval times for your applications.
-
Is there a cost associated with using airSlate SignNow for the Health Insurance Application For Extended Family Planning Benefits?
Yes, airSlate SignNow offers a variety of pricing plans to fit different organizational needs. Investing in airSlate SignNow for your Health Insurance Application For Extended Family Planning Benefits can save you time and resources, making it a cost-effective solution for managing your application process.
-
What benefits does airSlate SignNow offer for family planning health insurance applications?
Using airSlate SignNow for your Health Insurance Application For Extended Family Planning Benefits provides signNow benefits, including enhanced security, faster processing times, and easier document management. By automating the signing process, you can focus more on family planning and less on paperwork.
-
Can I integrate airSlate SignNow with other software for my health insurance applications?
Absolutely! airSlate SignNow offers seamless integrations with various software applications, allowing you to enhance your workflow when completing the Health Insurance Application For Extended Family Planning Benefits. This interoperability can help streamline your entire application process.
-
How secure is the Health Insurance Application For Extended Family Planning Benefits when using airSlate SignNow?
Security is a top priority at airSlate SignNow. When you use our platform for your Health Insurance Application For Extended Family Planning Benefits, your sensitive information is protected with industry-leading encryption and compliance standards, ensuring that your data remains safe.
Find out other health insurance application for extended family planning benefits form
- Close deals faster
- Improve productivity
- Delight customers
- Increase revenue
- Save time & money
- Reduce payment cycles
