
Fill and Sign the Printable 2020 Arkansas Form Ar1000 Od Organ Donor Donation
Useful Suggestions for Preparing Your ‘Printable 2020 Arkansas Form Ar1000 Od Organ Donor Donation’ Online
Are you fed up with the stress of handling paperwork? Look no further than airSlate SignNow, the premier electronic signature solution for individuals and organizations. Bid farewell to the monotonous routine of printing and scanning documents. With airSlate SignNow, you can effortlessly fill out and sign documents online. Take advantage of the comprehensive features embedded in this intuitive and budget-friendly platform and transform your document management process. Whether you need to authenticate forms or gather eSignatures, airSlate SignNow manages everything effortlessly, with just a few clicks.
Follow this comprehensive guide:
- Sign in to your account or initiate a free trial with our service.
- Click +Create to upload a file from your device, cloud, or our template collection.
- Open your ‘Printable 2020 Arkansas Form Ar1000 Od Organ Donor Donation’ in the editor.
- Click Me (Fill Out Now) to finalize the form on your end.
- Insert and designate fillable fields for others (if needed).
- Proceed with the Send Invite options to solicit eSignatures from others.
- Download, print your copy, or convert it into a reusable template.
Don't worry if you need to work with your colleagues on your Printable 2020 Arkansas Form Ar1000 Od Organ Donor Donation or send it for notarization—our platform has everything you need to complete such tasks. Create an account with airSlate SignNow today and elevate your document management to a new standard!
FAQs
-
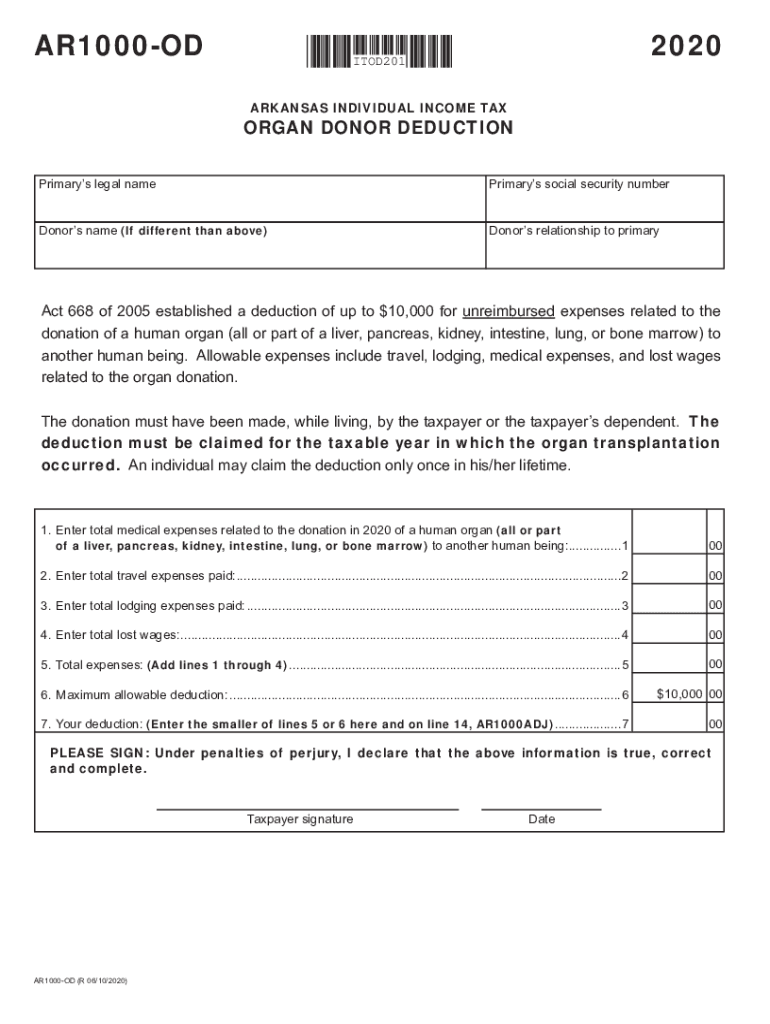
What is the Printable Arkansas Form AR1000 OD Organ Donor Donation?
The Printable Arkansas Form AR1000 OD Organ Donor Donation is a legal document that allows individuals to express their wish to donate their organs after death. This form is essential for ensuring your intentions are recognized and honored by medical professionals and family members.
-
How can I obtain the Printable Arkansas Form AR1000 OD Organ Donor Donation?
You can easily obtain the Printable Arkansas Form AR1000 OD Organ Donor Donation through airSlate SignNow's platform. Simply visit our site, and you can download the form in a printable format, making it convenient for you to fill out and submit.
-
Is there a fee associated with the Printable Arkansas Form AR1000 OD Organ Donor Donation?
The Printable Arkansas Form AR1000 OD Organ Donor Donation is available for free through airSlate SignNow. Our goal is to make the donation process accessible to everyone, so you can complete and print the form without any charges.
-
What are the benefits of using the Printable Arkansas Form AR1000 OD Organ Donor Donation?
Using the Printable Arkansas Form AR1000 OD Organ Donor Donation ensures that your wishes regarding organ donation are formally documented. This can provide peace of mind for you and your loved ones, knowing that your intentions will be respected and followed in the event of an emergency.
-
Can I fill out the Printable Arkansas Form AR1000 OD Organ Donor Donation online?
Yes, with airSlate SignNow, you can fill out the Printable Arkansas Form AR1000 OD Organ Donor Donation online. Our platform allows you to complete the form electronically, saving time and ensuring that all your information is accurately captured before printing.
-
How does airSlate SignNow ensure the security of my Printable Arkansas Form AR1000 OD Organ Donor Donation?
AirSlate SignNow prioritizes your security by using advanced encryption technology to protect your Printable Arkansas Form AR1000 OD Organ Donor Donation. Your personal information remains confidential and secure throughout the process, giving you peace of mind.
-
Can I save my Printable Arkansas Form AR1000 OD Organ Donor Donation for later?
Absolutely! With airSlate SignNow, you can save your Printable Arkansas Form AR1000 OD Organ Donor Donation as a draft. This feature allows you to return to complete the form at your convenience, ensuring that you can finalize it without any rush.
Find out other printable 2020 arkansas form ar1000 od organ donor donation
- Close deals faster
- Improve productivity
- Delight customers
- Increase revenue
- Save time & money
- Reduce payment cycles
