Annals of Oncology 14: 511–519, 2003
DOI: 10.1093/annonc/mdg167
Review
Control of cancer-related anemia with erythropoietic agents:
a review of evidence for improved quality of life and clinical
outcomes
D. Cella1*, D. Dobrez1 & J. Glaspy2
1
Institute for Health Services Research and Policy Studies, Northwestern University, Evanston, IL; 2Univeristy of California Los Angeles School of Medicine,
Los Angeles, CA, USA
Received 6 May 2002; revised 23 December 2002; accepted 15 January 2003
Background: Anemia occurs frequently in patients with cancer and is associated with impaired health-
Introduction
Anemia is a common occurrence in patients with cancer, particularly among those receiving myelosuppressive chemotherapy, in
whom anemia can occur in up to 100% of patients, depending on
the chemotherapy regimen used [1]. The incidence of anemia
varies depending upon the type of underlying malignancy, the
stage and duration of disease, the regimen and intensity of tumor
therapy, and possibly the occurrence of intercurrent infections or
surgery [2].
A number of factors may contribute to the development of
anemia, which is defined by the World Health Organization as a
hemoglobin level of ≤12 g/dl. Metastases within the bone
marrow may displace and destroy stem cells and progenitor cells,
which can damage the bone marrow microenvironment, impair
production of hematopoietic growth factors or induce production
*Correspondence to: Dr D. Cella, Center on Outcomes, Research and
Education, Evanston Northwestern Healthcare, 1001 University Place,
Suite 100, Evanston, IL 60201, USA. Tel: +1-847-570-7370;
Fax: +1-847-570-8033; E-mail: d-cella@northwestern.edu
© 2003 European Society for Medical Oncology
of cytokines that inhibit erythropoiesis [2]. These cytokines may
shorten red cell survival, induce a hypoproliferative state that
prevents the marrow from responding to hematopoietic demand
or cause a defect in iron re-utilization [2]. Where bone marrow
infiltration is not apparent, malignancy may induce anemia
through decreased production of erythropoietin [3]. Tumor bleeding, nutritional deficiencies and infections may also contribute to
the multifactorial etiology of anemia [4]. In addition, chemotherapy and radiotherapy may both contribute to the development
of anemia in patients with cancer [1, 2, 4–7]. This may be due to
the direct myelosuppressive effects of these therapies on the bone
marrow, or, in the case of platinum-containing agents, it may be
due to damage to erythropoietin-producing renal tubule cells.
Anemia may adversely affect patients with cancer in several
ways. This article critically reviews selected evidence demonstrating that correction of anemia with erythropoietic agents
improves health-related quality of life (HRQOL), and considers
specific data indicating that raising hemoglobin levels may
improve survival following cancer therapy. A better understanding of the way in which anemia affects patients with cancer
Downloaded from http://annonc.oxfordjournals.org/ by guest on September 6, 2014
related quality of life (HRQOL). Treatment of anemia results in significant improvements in energy, activity
and overall HRQOL, particularly among patients with mild-to-moderate anemia. Importantly, studies have
indicated that anemia may have a negative impact on the success of radiotherapy, reducing survival and
locoregional control. Recent preclinical and preliminary clinical data have also suggested that anemia may be
associated with poorer outcomes following chemotherapy or surgery.
Materials and methods: Data for review were identified and selected from searches of the literature
published from January 1990 through to October 2002 using Medline®, and searches of proceedings from key
international oncology and hematology meetings.
Results: A wealth of data indicate that treatment of anemia improves HRQOL in patients with cancer.
Prospective studies exploring survival and/or treatment outcomes in anemic cancer patients are currently in
their early stages, preventing any firm conclusions from being drawn, although they do indicate a benefit in
treating anemia.
Conclusions: Recent studies support the use of erythropoietic agents in anemic cancer patients as a means
of raising their hemoglobin levels and consequently improving their HRQOL. Randomized, controlled trials
are needed to determine whether treating anemia with erythropoietic agents will improve other outcomes
following therapy.
Key words: anemia, cancer, darbepoetin α, health-related quality of life, recombinant human
erythropoietin, survival
�512
should facilitate informed decisions regarding the appropriate
management of anemia.
Materials and methods
Impact of anemia on HRQOL
Decreased oxygen delivery to tissues can result from anemia,
which may adversely affect virtually all organs [8]. Anemia is a
multi-symptom syndrome, with fatigue being the primary symptom. Other manifestations include exertional dyspnea, cardiovascular complications, dizziness, headache, chest pain, decreased
motivation and depression, impaired cognitive function, anorexia,
nausea, indigestion, sleeping disorders, menstrual problems and
loss of libido [9]. Symptom severity depends on the degree of
anemia, as well as the rapidity of its onset, and the patient’s
pulmonary and cardiovascular function. Obviously, these symptoms also impact on HRQOL, and several studies have documented the effects of anemia on the lives of patients with cancer
[10–13].
Although care should be taken when making clinical interpretations from results generated by any HRQOL assessment, a
number of tools to measure HRQOL in patients with cancer have
become widely used and accepted. One of these, the Functional
Assessment of Cancer Therapy-Anemia (FACT-An) scale, was
developed specifically to assess the impact of anemia on patients
[10]. Other tools frequently used include the Linear Analog Scale
Assessment (LASA) and the Functional Assessment of Cancer
Therapy-Fatigue (FACT-F) scale. These tools provide a useful
measure of energy levels and ability to perform daily tasks as
well as physical, social and emotional well-being in patients with
cancer.
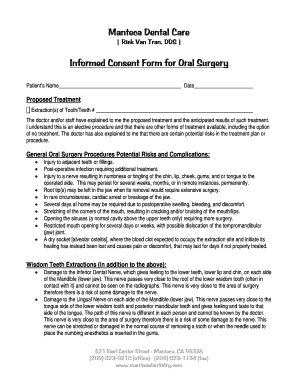
Health-related quality of life has been shown to correlate
directly with the degree of anemia in patients with cancer [10,
11]. Figure 1 shows the relationship between HRQOL (measured
using the FACT-An scale) and hemoglobin levels [10]. The
patient’s ability to work is also associated with hemoglobin
levels. In one study, 25% of patients with hemoglobin levels
≤12 g/dl reported that they were unable to work, compared with
only 8% of patients with hemoglobin levels >12 g/dl [11]. Overall,
Figure 1. The association between health-related quality of life [as
measured by the Functional Assessment of Cancer Therapy-Anemia
(FACT-An) scale] and hemoglobin level in cancer patients with anemia
[10].
patients with hemoglobin levels >12 g/dl have reported significantly less fatigue and other symptoms of anemia, better physical
and functional well-being, and higher general HRQOL [11].
Anemia and fatigue
Fatigue can be defined as the subjective sensation of having
reduced energy, loss of strength or becoming easily tired [14].
Several researchers have assessed the prevalence, consequences
and perceptions of fatigue in patients with cancer, caregivers and
oncologists [15–17]. They found that more than three-quarters of
patients with cancer experienced fatigue, defined for the purposes of these studies as debilitating tiredness during the course
of their disease and treatment [15]. Of the patients reporting
fatigue in a study by Curt et al. [16], 91% said that it prevented
them from leading a ‘normal’ life and 88% indicated that fatigue
altered their daily routine.
Fatigue is often attributed to low hemoglobin levels [9]. However, anemia is not the only cause of fatigue and the precise
relationship between hemoglobin level and fatigue is not well
understood [14]. Nevertheless, hemoglobin levels should be evaluated when patients present with fatigue, as therapy for anemia
is available.
Treating anemia associated with cancer
Anemia in patients with cancer is primarily treated with red blood
cell transfusions, or administration of erythropoietic proteins.
Blood transfusions provide rapid relief from anemia but are
associated with many real and perceived risks, such as infections
and hemolytic reactions [18]. Furthermore, patients often prefer
to avoid these procedures [18].
Epoetin (α/β) effectively raises hemoglobin levels and
decreases transfusion requirements in 50–60% of patients with
anemia of cancer [19–21]. Increased hemoglobin levels and
decreased transfusions have also been reported following treatment with darbepoetin α, a novel erythropoiesis stimulating protein with a longer serum half-life than epoetin [22–25]. However,
Downloaded from http://annonc.oxfordjournals.org/ by guest on September 6, 2014
Potential data for review were identified from searches of the published
literature using Medline® and proceedings from international oncology and
hematology meetings (American Society of Hematology/American Society
of Clinical Oncology/European Cancer Conference). The searches were
limited to abstracts/articles in English, involving human adult subjects and
published from January 1990 to October 2002. The text words ‘cancer,
anemia, and quality of life’ were used in the title, abstracts or keyword list
search for evidence relating to HRQOL. For data relating to anemia and
cancer therapy outcomes the following text words were used in the search:
‘cancer, hemoglobin, local control, impact, and chemoradiation’. Key references, which reported original study results of direct relevance to the topic
discussed, were then selected for review. Only prospective studies analyzing
HRQOL were selected, while retrospective analysis on anemia and cancer
therapy outcomes were also reviewed, due to the low number of prospective
trials on this subject. The majority of studies selected for review were also
found to be industry supported. It should be noted that in such studies, there is
the potential for some bias in the selection of endpoints.
�513
These studies utilize a high-dose loading phase with the aim of
inducing an initial rapid hematological response, followed by a
lower-dose maintenance phase to sustain the response.
Treating anemia with erythropoietic agents
improves HRQOL
Numerous placebo-controlled and open-label studies have demonstrated that measurable improvements in HRQOL can be
achieved through the treatment of anemia with erythropoiesis
stimulating proteins in patients with cancer [12, 13, 19–22, 37–
39]. The US Cancer Pain Relief Committee recently analyzed
five randomized, placebo-controlled trials and two large, openlabel trials, published between 1990 and 2001, to confirm the
beneficial effects of epoetin on HRQOL in anemic cancer
patients. From this analysis, evidence-based guidelines have
been proposed that recommend epoetin as a safe and effective
treatment that should be used in patients for whom symptoms of
anemia are sufficient to impair functional capacity or HRQOL,
where the anemia is sufficient to necessitate blood transfusion, or
if blood transfusion is not an acceptable treatment option [40].
Similarly, the evidence-based review commissioned by the
Agency for Healthcare Research and Quality recommends that
epoetin is effective in reducing transfusion risk among anemic
(hemoglobin declining to near 10 g/dl) cancer patients receiving
chemotherapy. This report also concluded that available quality
of life data from adequately powered, methodologically rigorous
studies were not yet sufficient to support the quality of life benefits from epoetin therapy in this setting [41]. However, since this
analysis, which considered data published up until the end of
1999, data from prospective trials assessing HRQOL by validated questionnaires in patients with cancer receiving erythropoietic agents have been published. These more recent trials, which
were considered in the US Cancer Pain Relief Committee analysis, demonstrate significant improvements in HRQOL following
treatment of anemia with an erythropoietic protein [38, 39, 42].
Most recently, another placebo-controlled trial of epoetin α therapy during cancer chemotherapy has been reported, demonstrating a greater improvement in FACT-F score in the treatment
group [43]. We believe that these additional studies, published
since the meta-analysis by the Agency for Healthcare Research
and Quality, demonstrate the HRQOL benefits of anemia therapy
in patients with cancer.
In a recent, double-blind, placebo-controlled trial involving
375 patients with non-myeloid malignancies, administration of
150–300 U/kg epoetin α three times a week for 12–24 weeks
resulted in a significant decrease in red blood cell transfusion
requirements. Twenty-five per cent of patients receiving epoetin
α required a transfusion after day 28, compared with 40% of
placebo patients (P = 0.0057). Patients receiving epoetin α also
experienced a significant increase in hemoglobin compared with
patients receiving placebo (2.2 versus 0.5 g/dl; P < 0.001). In
addition, compared with placebo-treated patients, patients receiving epoetin α reported significant increases in energy levels
(epoetin α +8.1; placebo –5.8; P = 0.007), ability to carry out
daily activities (epoetin α +7.5; placebo –6.0; P = 0.0018) and
Downloaded from http://annonc.oxfordjournals.org/ by guest on September 6, 2014
the cost-effectiveness of these erythropoietic proteins has not yet
been demonstrated. Published studies have differed significantly
in their design and perspective, inclusion of indirect costs (such
as patient travel time), their choice of a primary outcome variable
and their treatment of HRQOL effects. Comparison across studies is therefore difficult. Cost-effectiveness studies, conducted
from a healthcare system perspective, found that epoetin therapy
was not cost-effective relative to the use of transfusions [26, 27].
Transfusion therapy was found to be cost-saving relative to epoetin in the study by Sheffield et al. [26], while in a study by Barosi
et al. [27] the marginal cost of epoetin therapy relative to standard
care was estimated to be US $189652 per quality-adjusted life
year, an amount generally not considered to be cost-effective
[27]. A further study by Ortega et al. [28] demonstrated that
patients in Canada were willing to pay far less on average than the
incremental cost of erythropoietin (including both direct medical
costs plus patient travel time for the purpose of receiving a transfusion), resulting in a net incremental treatment cost of at least
US $2943. However, other research has suggested that the use of
epoetin therapy may be cost-effective relative to standard care. A
modeling study conducted from the provider perspective by
Cremieux et al. [29] drew direct medical cost and effectiveness
assumptions from a literature review and three US clinical trials
involving more than 4500 patients with cancer. Using cumulative
change in hemoglobin levels for a 16-week treatment period, the
study showed that the effectiveness from US $1 spent on standard
care could be achieved with US $0.81 using epoetin therapy. The
estimated cost-effectiveness of epoetin therapy relative to transfusion is dependent on multiple study design issues, and is in
need of further evaluation. Reduced administration costs and
improved targeting of epoetin therapy to those most likely to
benefit from the treatment could improve the cost-effectiveness
of its use.
Research conducted in 3472 cancer patients from 1996 to 2000
suggests that as few as 30% of patients in the USA receive epoetin treatment for anemia despite the high incidence of anemia in
patients with cancer and the known benefits of therapy [30]. Furthermore, a recent survey of physicians in the USA showed that
anemia remains under-treated across all hemoglobin levels, with
only 35% and 15% of patients with hemoglobin levels of