
Fill and Sign the Long Term Care Insurance Policy Illustration Form
Valuable instructions on preparing your ‘Long Term Care Insurance Policy Illustration Form’ online
Are you fed up with the inconvenience of handling paperwork? Look no further than airSlate SignNow, the leading electronic signature platform for individuals and small to medium-sized businesses. Bid farewell to the tedious routine of printing and scanning documents. With airSlate SignNow, you can easily finalize and authorize paperwork online. Take advantage of the comprehensive tools embedded in this user-friendly and budget-friendly platform and transform your method of paperwork handling. Whether you need to approve documents or gather eSignatures, airSlate SignNow manages it all effortlessly, requiring only a few clicks.
Adhere to this detailed guide:
- Log into your account or register for a complimentary trial with our service.
- Click +Create to upload a file from your device, cloud storage, or our template library.
- Open your ‘Long Term Care Insurance Policy Illustration Form’ in the editor.
- Click Me (Fill Out Now) to prepare the document on your end.
- Add and assign fillable fields for other users (if necessary).
- Proceed with the Send Invite settings to solicit eSignatures from others.
- Save, print your copy, or convert it into a multi-use template.
Don’t be concerned if you need to collaborate with your teammates on your Long Term Care Insurance Policy Illustration Form or send it for notarization—our solution provides everything needed to accomplish such tasks. Establish an account with airSlate SignNow today and elevate your document management to a new level!
FAQs
-
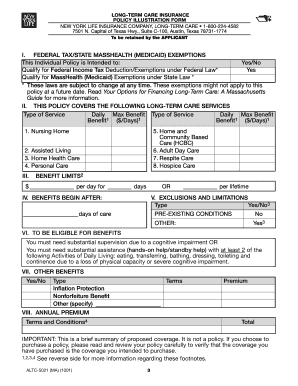
What is a Long Term Care Insurance Policy Illustration Form?
The Long Term Care Insurance Policy Illustration Form is a document that provides a detailed projection of potential benefits and costs associated with a long-term care insurance policy. This illustration helps policyholders understand how their coverage can support them in the future, ensuring they make informed decisions about their long-term care needs.
-
How can I obtain a Long Term Care Insurance Policy Illustration Form?
You can easily obtain a Long Term Care Insurance Policy Illustration Form through your insurance provider or directly on our platform. By using airSlate SignNow, you can request and receive the form electronically, making it quick and convenient to access the necessary information regarding your long-term care policy.
-
What information is included in a Long Term Care Insurance Policy Illustration Form?
A Long Term Care Insurance Policy Illustration Form typically includes details about premium costs, benefit amounts, and the duration of coverage. Additionally, it may outline different scenarios of care needs and how the policy will respond, helping you visualize your options for long-term care.
-
Is there a cost associated with the Long Term Care Insurance Policy Illustration Form?
Most insurance providers offer the Long Term Care Insurance Policy Illustration Form at no additional cost to their clients. Using airSlate SignNow, you can access this form without incurring extra fees, allowing you to evaluate your policy options without financial pressure.
-
How does airSlate SignNow streamline the process of obtaining a Long Term Care Insurance Policy Illustration Form?
airSlate SignNow simplifies the process by enabling users to request and eSign the Long Term Care Insurance Policy Illustration Form online. This digital solution eliminates the need for physical paperwork, ensuring a fast and efficient experience for both policyholders and insurance agents.
-
What are the benefits of using the Long Term Care Insurance Policy Illustration Form?
Using the Long Term Care Insurance Policy Illustration Form provides clear insights into your potential long-term care costs and benefits. This transparency allows you to compare different policies, assess your needs, and plan for future care, making it a crucial tool for financial planning.
-
Can I integrate the Long Term Care Insurance Policy Illustration Form with other tools?
Yes, airSlate SignNow allows seamless integration with various tools and platforms to enhance your workflow. You can easily link the Long Term Care Insurance Policy Illustration Form with CRM systems and other applications to streamline document management and client communication.
Find out other long term care insurance policy illustration form
- Close deals faster
- Improve productivity
- Delight customers
- Increase revenue
- Save time & money
- Reduce payment cycles
