
Fill and Sign the Arkansas State Board of Cosmetolgy New Establishment Application Form
Useful tips for finalizing your ‘Arkansas State Board Of Cosmetolgy New Establishment Application Form’ online
Are you fed up with the burden of handling paperwork? Look no further than airSlate SignNow, the premier eSignature platform for both individuals and businesses. Bid farewell to the lengthy procedure of printing and scanning documents. With airSlate SignNow, you can effortlessly complete and sign documents online. Utilize the robust features incorporated into this user-friendly and affordable platform and transform your method of paperwork management. Whether you need to sign forms or collect eSignatures, airSlate SignNow makes it simple, requiring only a few clicks.
Follow this comprehensive guide:
- Log into your account or sign up for a complimentary trial with our service.
- Click +Create to upload a file from your device, cloud storage, or our form collection.
- Open your ‘Arkansas State Board Of Cosmetolgy New Establishment Application Form’ in the editor.
- Click Me (Fill Out Now) to set up the document on your end.
- Add and assign fillable fields for others (if necessary).
- Proceed with the Send Invite options to solicit eSignatures from others.
- Save, print your copy, or convert it into a reusable template.
Don’t fret if you need to work with others on your Arkansas State Board Of Cosmetolgy New Establishment Application Form or send it for notarization—our platform offers all the tools you need to achieve those goals. Register for an account with airSlate SignNow today and elevate your document management to a new standard!
FAQs
-
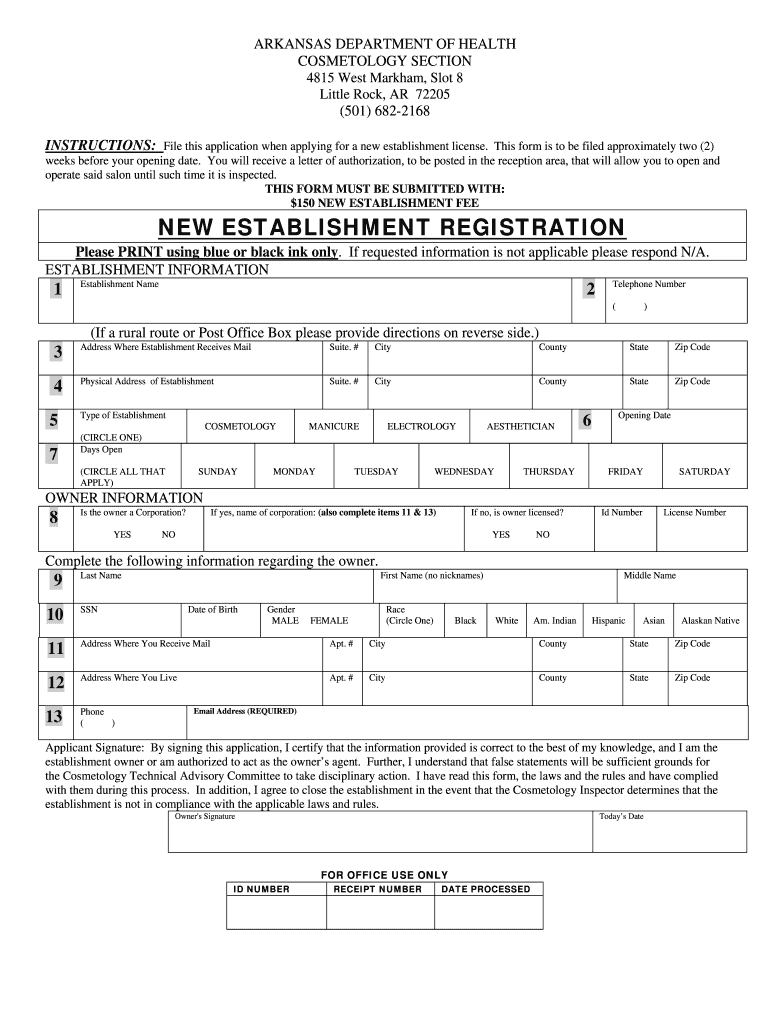
What is the Arkansas State Board Of Cosmetology New Establishment Application Form?
The Arkansas State Board Of Cosmetology New Establishment Application Form is a necessary document for businesses seeking to establish a cosmetology practice in Arkansas. This form ensures that your establishment complies with state regulations and standards, paving the way for a successful launch of your beauty or cosmetology services.
-
How can airSlate SignNow help with the Arkansas State Board Of Cosmetology New Establishment Application Form?
airSlate SignNow streamlines the completion and submission of the Arkansas State Board Of Cosmetology New Establishment Application Form. With our easy-to-use eSignature solution, you can fill out, sign, and send your application quickly, ensuring you meet all necessary deadlines without hassle.
-
Is there a fee for submitting the Arkansas State Board Of Cosmetology New Establishment Application Form?
Yes, there is typically a fee associated with submitting the Arkansas State Board Of Cosmetology New Establishment Application Form. The exact amount may vary, so it’s advisable to check the Arkansas State Board of Cosmetology’s official website for the latest fee structure and payment methods.
-
What features does airSlate SignNow offer for completing the Arkansas State Board Of Cosmetology New Establishment Application Form?
airSlate SignNow offers a range of features designed to simplify the completion of the Arkansas State Board Of Cosmetology New Establishment Application Form. These include customizable templates, secure eSignatures, and document tracking to ensure that your application process is smooth and efficient.
-
Can I integrate airSlate SignNow with other software to manage my Arkansas State Board Of Cosmetology New Establishment Application Form?
Absolutely! airSlate SignNow integrates seamlessly with various business applications, allowing you to manage your Arkansas State Board Of Cosmetology New Establishment Application Form alongside other tools you use. This integration helps streamline your workflow by connecting your documents with your favorite CRM, project management, or accounting software.
-
What are the benefits of using airSlate SignNow for my Arkansas State Board Of Cosmetology New Establishment Application Form?
Using airSlate SignNow for your Arkansas State Board Of Cosmetology New Establishment Application Form offers numerous benefits, including increased efficiency and reduced paperwork. Our platform ensures that your documents are securely stored and easily accessible, allowing for faster processing and submission of your application.
-
Is airSlate SignNow secure for handling the Arkansas State Board Of Cosmetology New Establishment Application Form?
Yes, airSlate SignNow prioritizes security and compliance, making it a safe choice for handling your Arkansas State Board Of Cosmetology New Establishment Application Form. We utilize industry-standard encryption and security protocols to protect your sensitive information throughout the signing and submission process.
Related searches to arkansas state board of cosmetolgy new establishment application form
Find out other arkansas state board of cosmetolgy new establishment application form
- Close deals faster
- Improve productivity
- Delight customers
- Increase revenue
- Save time & money
- Reduce payment cycles
