Social Security Administration Form Approved
Please read the back of the last copy before you complete this form. OMB No. 0960-0527
Name (Claimant) (Print or Type)
Wage Earner (If Different)
Social Security Number
Social Security Number
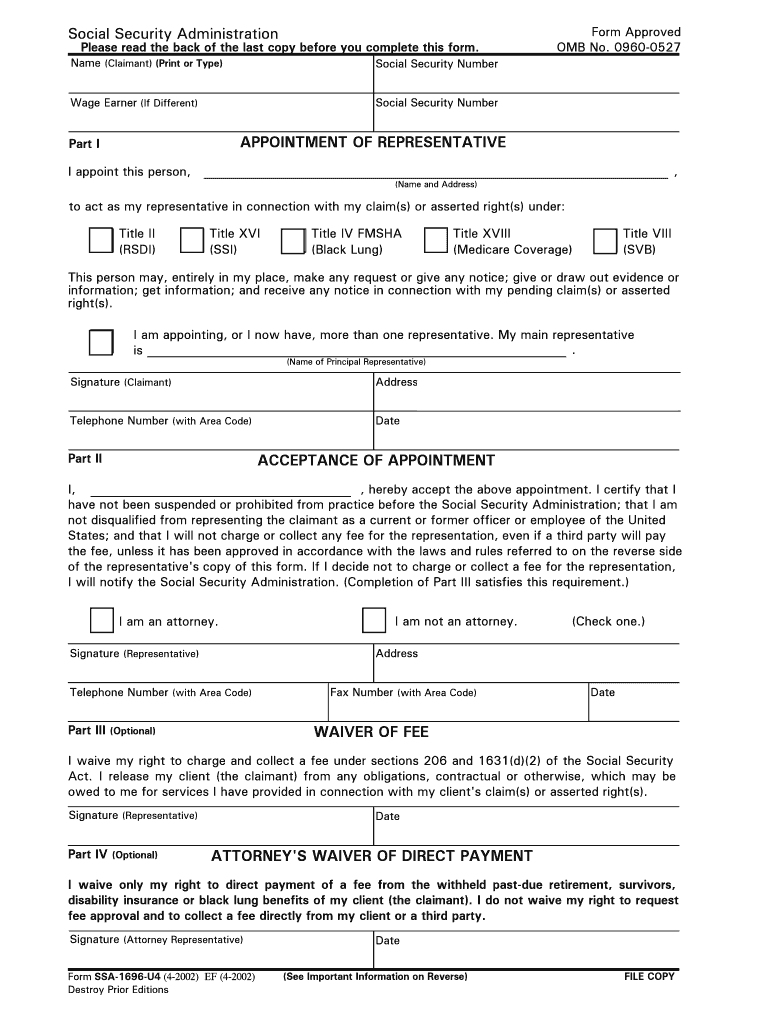
Part I APPOINTMENT OF REPRESENTATIVE
I appoint this person, (Name and Address)
to act as my representative in connection with my claim(s) or asserted right(s) under:
Title II Title XVI Title IV FMSHA Title XVIII
(RSDI) (SSI) (Black Lung) (Medicare Coverage) ,
Title VIII (SVB)
This person may, entirely in my place, make any request or give any notice; give or draw out evidence or
information; get information; and receive any notice in connection with my pending claim(s) or asserted
right(s).
I am appointing, or I now have, more than one representative. My main representative is .
(Name of Principal Representative)
Signature (Claimant)
Telephone Number (with Area Code) Address
Date
Part II
ACCEPTANCE OF APPOINTMENT
I, , hereby accept the above appointment. I certify that I
have not been suspended or prohibited from prac
tice before the Social Security Administration; that I am
not disqualified from representing the claimant as a current or former officer or employee of the United States; and that I will not charge or collect any fee for the representation, even if a third party will pay
the fee, unless it has been approved in accordance with the laws and rules referred to on the reverse side
of the representative's copy of this form. If I decide not to charge or collect a fee for the representation, I will notify the Social Security Administration. (Completion of Part III satisfies this requirement.)
I am an attorney. I am not an attorney.
(Check one.)
Signature (Representative)
Telephone Number (with Area Code)
Address
Date Fax Number (with Area Code)
Part III (Optional)
WAIVER OF FEE
I waive my right to charge and collect a fee under sections 206 and 1631(d)(2) of the Social Security
Act. I release my client (the claimant) from any obligations, contractual or otherwise, which may be owed to me for services I have provided in connection with my client's claim(s) or asserted right(s).
Signature (Representative) Date
Part IV (Optional)
ATTORNEY'S WAIVER OF DIRECT PAYMENT
I waive only my right to direct payment of a fee from the withheld past-due retirement, survivors,
disability insurance or black lung benefits of my client (the claimant). I do not waive my right to request fee approval and to collect a fee directly from my client or a third party.
Signature (Attorney Representative) Date
Form SSA-1696-U4 (4-2002) EF (4-2002) (See Important Information on Reverse)
FILE COPY
Destroy Prior Editions
INFORMATION FOR CLAIMANTS
What A Representative May Do
We will work directly with your appointed representative
unless he or she asks us to work directly with you. Your representative may:
o get information from your claim(s) file;
o give us evidence or information to support your claim; o come with you, or for you, to any interview,
conference, or hearing you have with us;
o request a reconsideration, hearing, or Appeals Council
review; and
o
help you and your witnesses prepare for a hearing and
question any witnesses.
Also, your representative will receive a copy of the
decision(s) we make on your claim(s). We will rely on your representative to tell you about the status of your claim(s),
but you still may call or visit us for information.
You and your representative(s) are responsible for giving
Social Security accurate information. It is wrong to
knowingly and willingly furnish false information. Doing so
may result in criminal prosecution.
We usually continue to work with your representative until
(1) you tell us that he or she no longer represents you; or
(2) your representative tells us that he or she is withdrawing
or indicates that his or her services have ended (for example, by filing a fee petition or not pursuing an appeal). We do not continue to work with someone who is suspended
or disqualified from representing claimants.
What Your Representative(s) May Charge
Each representative you appoint can ask for a fee. To charge
you a fee for services, your representative must get our
approval. (Even when someone else will pay the fee for you,
for example, an insurance company, your representative
usually must get our approval.) One way is to file a fee
petition. The other way is to file a fee agreement with us. In
either case, your representative cannot charge you more than
the fee amount we approve. If he or she does, promptly
report this to your Social Security office.
o Filing A Fee Petition
Your representative may ask for approval of a fee by
giving us a fee petition when his or her work on your
claim(s) is complete. This written request describes in
detail the amount of time he or she spent on each service
provided you. The request also gives the amount of the
fee the representative wants to charge for these services.
Your representative must give you a copy of the fee
petition and each attachment. If you disagree with the
information shown in the fee petition, contact your
Social Security office. Please do this within 20 days of
receiving your copy of the petition.
We will review the petition and consider the reasonable
value of the services provided. Then we will tell you in
writing the amount of the fee we approve.
Form SSA-1696-U4 (4-2002) EF (4-2002) What Your Representative(s) May Charge,
continued o
Filing
A Fee Agreement
If you and your representative have a written fee
agreement, one of you must give it to us before we decide
your claim(s). We usually will approve the agreement if
you both signed it; the fee you agreed on is no more than
25 percent of past-due benefits, or $5,300 (or a higher
amount we set and announce in the Federal Register),
whichever is less; we approve your claim(s); and your
claim results in past-due benefits. We will tell you in
writing the amount of the fee your representative can
charge based on the agreement.
If we do not approve the fee agreement, we will tell you
and your representative in writing. Then your
representative must file a fee petition to charge and collect
a fee.
After we tell you the amount of the fee your representative
can charge, you or your representative can ask us to look at it
again if either or both of you disagree with the amount. (If we
approved a fee agreement, the person who decided your
claim(s) also may ask us to lower the amount.) Someone who did not decide the amount of the fee the first time will review
and finally decide the amount of the fee.
How Much You Pay
You never owe more than the fee we approve, except for:
o any fee a Federal court allows for your representative's services before it; and
o out-of-pocket expenses your representative incurs or expects to incur, for example, the cost of getting your
doctor's or hospital records. Our approval is not
needed for such expenses.
Your representative may accept money in advance as long as
he or she holds it in a trust or escrow account. If an attorney
represents you and your retirement, survivors, disability
insurance, or black lung claim results in past-due benefits, we
usually withhold 25 percent of your past-due benefits to pay toward the fee for you.
You must pay your representative directly:
o the rest of the fee you owe - if the amount of the fee is more than any amount(s)
your representative held for you in a trust or escrow
account and we withheld and paid your attorney for you.
o all of the fee you owe
- if we did not withhold past-due benefits, for
example, when your representative is not an
attorney or the benefits are supplemental security income; or
- if we withheld, but later paid you the money
because your attorney did not either ask for our
approval until after 60 days of the date of your
notice of award or tell us on time that he or she
planned to ask for a fee.
Social Security Administration Form Approved
Please read the back of the last copy before you complete this form. OMB No. 0960-0527
Name (Claimant) (Print or Type)
Wage Earner (If Different)
Social Security Number
Social Security Number
Part I APPOINTMENT OF REPRESENTATIVE
I appoint this person, ,
(Name and Address)
to act as my representative in connection with my claim(s) or asserted right(s) under:
Title II Title XVI Title IV FMSHA Title XVIII Title VIII
(RSDI) (SSI) (Black Lung) (Medicare Coverage) (SVB)
This person may, entirely in my place, make any request or give any notice; give or draw out evidence or
information; get information; and receive any notice in connection with my pending claim(s) or asserted
right(s).
I am appointing, or I now have, more than one representative. My main representative is .
(Name of Principal Representative)
Signature (Claimant)
Telephone Number (with Area Code) Address
Date
Part II ACCEPTANCE OF APPOINTMENT
I, , hereby accept the above appointment. I certify that I
have not been suspended or prohibited from practice before the Social Security Administration; that I am
not disqualified from representing the claimant as a current or former officer or employee of the United States; and that I will not charge or collect any fee for the representation, even if a third party will pay
the fee, unless it has been approved in accordance with the laws and rules referred to on the reverse side
of the representative's copy of this form. If I decide not to charge or collect a fee for the representation, I will notify the Social Security Administration. (Completion of Part III satisfies this requirement.)
I am an attorney. I am not an attorney.
(Check one.)
Signature (Representative) Address
Telephone Number (with Area Code) Date Fax Number (with Area Code)
Part III (Optional)
WAIVER OF FEE
I waive my right to charge and collect a fee under sections 206 and 1631(d)(2) of the Social Security Act. I release my client (the claimant) from any obligations, contractual or otherwise, which may be owed to me for services I have provided in connection with my client's claim(s) or asserted right(s).
Signature (Representative) Date
Part IV (Optional)
ATTORNEY'S WAIVER OF DIRECT PAYMENT
I waive only my right to direct payment of a fee from the withheld past-due retirement, survivors,
disability insurance or black lung benefits of my client (the claimant). I do not waive my right to request fee approval and to collect a fee directly from my client or a third party.
Signature (Attorney Representative) Date
Form SSA-1696-U4 (4-2002) EF (4-2002) (See Important Information on Reverse)
CLAIMANT'S COPY
Destroy Prior Editions
INFORMATION FOR CLAIMANTS
What A Representative May Do
We will work directly with your appointed representative
unless he or she asks us to work directly with you. Your representative may:
o get information from your claim(s) file;
o give us evidence or information to support your claim; o come with you, or for you, to any interview,
conference, or hearing you have with us;
o request a reconsideration, hearing, or Appeals Council
review; and
o
help you and your witnesses prepare for a hearing and
question any witnesses.
Also, your representative will receive a copy of the
decision(s) we make on your claim(s). We will rely on your representative to tell you about the status of your claim(s),
but you still may call or visit us for information.
You and your representative(s) are responsible for giving
Social Security accurate information. It is wrong to
knowingly and willingly furnish false information. Doing so
may result in criminal prosecution.
We usually continue to work with your representative until
(1) you tell us that he or she no longer represents you; or
(2) your representative tells us that he or she is withdrawing
or indicates that his or her services have ended (for example, by filing a fee petition or not pursuing an appeal). We do not continue to work with someone who is suspended
or disqualified from representing claimants.
What Your Representative(s) May Charge
Each representative you appoint can ask for a fee. To charge
you a fee for services, your representative must get our
approval. (Even when someone else will pay the fee for you,
for example, an insurance company, your representative
usually must get our approval.) One way is to file a fee
petition. The other way is to file a fee agreement with us. In
either case, your representative cannot charge you more than
the fee amount we approve. If he or she does, promptly
report this to your Social Security office.
o Filing A Fee Petition
Your representative may ask for approval of a fee by
giving us a fee petition when his or her work on your
claim(s) is complete. This written request describes in
detail the amount of time he or she spent on each service
provided you. The request also gives the amount of the
fee the representative wants to charge for these services.
Your representative must give you a copy of the fee
petition and each attachment. If you disagree with the
information shown in the fee petition, contact your
Social Security office. Please do this within 20 days of
receiving your copy of the petition.
We will review the petition and consider the reasonable
value of the services provided. Then we will tell you in
writing the amount of the fee we approve.
Form SSA-1696-U4 (4-2002) EF (4-2002) What Your Representative(s) May Charge,
continued o
Filing
A Fee Agreement
If you and your representative have a written fee
agreement, one of you must give it to us before we decide
your claim(s). We usually will approve the agreement if
you both signed it; the fee you agreed on is no more than
25 percent of past-due benefits, or $5,300 (or a higher
amount we set and announce in the Federal Register),
whichever is less; we approve your claim(s); and your
claim results in past-due benefits. We will tell you in
writing the amount of the fee your representative can
charge based on the agreement.
If we do not approve the fee agreement, we will tell you
and your representative in writing. Then your
representative must file a fee petition to charge and collect
a fee.
After we tell you the amount of the fee your representative
can charge, you or your representative can ask us to look at it
again if either or both of you disagree with the amount. (If we
approved a fee agreement, the person who decided your
claim(s) also may ask us to lower the amount.) Someone who did not decide the amount of the fee the first time will review
and finally decide the amount of the fee.
How Much You Pay
You never owe more than the fee we approve, except for:
o any fee a Federal court allows for your representative's services before it; and
o out-of-pocket expenses your representative incurs or expects to incur, for example, the cost of getting your
doctor's or hospital records. Our approval is not
needed for such expenses.
Your representative may accept money in advance as long as
he or she holds it in a trust or escrow account. If an attorney
represents you and your retirement, survivors, disability
insurance, or black lung claim results in past-due benefits, we
usually withhold 25 percent of your past-due benefits to pay toward the fee for you.
You must pay your representative directly:
o the rest of the fee you owe - if the amount of the fee is more than any amount(s)
your representative held for you in a trust or escrow
account and we withheld and paid your attorney for you.
o all of the fee you owe
- if we did not withhold past-due benefits, for
example, when your representative is not an
attorney or the benefits are supplemental security income; or
- if we withheld, but later paid you the money
because your attorney did not either ask for our
approval until after 60 days of the date of your
notice of award or tell us on time that he or she
planned to ask for a fee.
Social Security Administration Form Approved
Please read the back of the last copy before you complete this form. OMB No. 0960-0527
Name (Claimant) (Print or Type)
Wage Earner (If Different)
Social Security Number
Social Security Number
Part I APPOINTMENT OF REPRESENTATIVE
I appoint this person, ,
(Name and Address)
to act as my representative in connection with my claim(s) or asserted right(s) under:
Title II Title XVI Title IV FMSHA Title XVIII Title VIII
(RSDI) (SSI) (Black Lung) (Medicare Coverage) (SVB)
This person may, entirely in my place, make any request or give any notice; give or draw out evidence or
information; get information; and receive any notice in connection with my pending claim(s) or asserted
right(s).
I am appointing, or I now have, more than one representative. My main representative is .
(Name of Principal Representative)
Signature (Claimant) Address
Part II ACCEPTANCE OF APPOINTMENT
I, , hereby accept the above appointment. I certify that I
have not been suspended or prohibited from practice before the Social Security Administration; that I am
not disqualified from representing the claimant as a current or former officer or employee of the United States; and that I will not charge or collect any fee for the representation, even if a third party will pay
the fee, unless it has been approved in accordance with the laws and rules referred to on the reverse side
of the representative's copy of this form. If I decide not to charge or collect a fee for the representation, I will notify the Social Security Administration. (Completion of Part III satisfies this requirement.)
I am an attorney. I am not an attorney.
(Check one.)
Fax Number (with Area Code)
Signature (Representative)
Telephone Number (with Area Code) Address
Date
Part III (Optional)
WAIVER OF FEE
I waive my right to charge and collect a fee under sections 206 and 1631(d)(2) of the Social Security Act. I release my client (the claimant) from any obligations, contractual or otherwise, which may be owed to me for services I have provided in connection with my client's claim(s) or asserted right(s).
Signature (Representative) Date
Part IV (Optional)
ATTORNEY'S WAIVER OF DIRECT PAYMENT
I waive only my right to direct payment of a fee from the withheld past-due retirement, survivors,
disability insurance or black lung benefits of my client (the claimant). I do not waive my right to request fee approval and to collect a fee directly from my client or a third party.
Signature (Attorney Representative) Date
Form SSA-1696-U4 (4-2002) EF (4-2002) (See Important Information on Reverse)
REPRESENTATIVE'S COPY
Destroy Prior Editions
INFORMATION FOR REPRESENTATIVES
Fees For Representation
An attorney or other person who wants to charge or
collect a fee for providing services in connection with a claim before the Social Security Administration must first
obtain our approval of the fee for representation. The only
exceptions are if the fee is for services provided:
o
when a nonprofit organization or government
agency will pay the fee and any expenses from
government funds and the claimant incurs no
liability, directly or indirectly, for the cost(s);
o
in an official capacity such as legal guardian,
committee, or similar court-appointed office and
the court has approved the fee in question; or
o in representing the claimant before a court of
law. A representative who has provided
services in a claim before both the Social
Security Administration and a court of law may
seek a fee from either or both, but neither tribunal has the authority to set a fee for
services provided before the other.
Obtaining Approval Of A Fee
To charge a fee for services, you must use one of two,
mutually exclusive fee approval processes. You must file
either a fee petition or a fee agreement with us. In either
case, you cannot charge more than the fee amount we approve.
o Fee Petition Process
You may ask for approval of a fee by giving us a fee
petition when you have completed your services to the
claimant. This written request must describe in detail
the amount of time you spent on each service provided
and the amount of the fee you are requesting.
You must give the claimant a copy of the fee petition
and each attachment. The claimant may disagree with
the information shown by contacting a Social Security
office within 20 days of receiving his or her copy of
the fee petition. We will consider the reasonable value
of the services provided, and send you notice of the
amount of the fee you can charge.
o Fee Agreement Process
If you and the claimant have a written fee agreement,
either of you must give it to us before we decide the
claim(s). We usually will approve the agreement if
you both signed it; the fee you agreed on is no more
than 25 percent of past-due benefits, or $5,300 (or a higher amount we set and announce in the Federal
Register), whichever is less; we approve the
claim(s); and the claim results in past-due benefits.
We will send you a copy of the notice we send the
claimant telling him or her the amount of the fee you
can charge based on the agreement.
If we do not approve the fee agreement, we will tell you in writing. We also will tell you and the claimant
that you must file a fee petition if you wish to charge
and collect a fee.
After we tell you the amount of the fee you can charge, you
or the claimant may ask us in writing to review the approved
fee. (If we approved a fee agreement, the person who
decided the claim(s) also may ask us to lower the amount.)
Someone who did not decide the amount of the fee the first time will review and finally decide the amount of the fee. Collecting A Fee
You may accept money in advance, as long as you hold it in a trust or escrow account. The claimant never owes you
more than the fee we approve, except for:
o any fee a Federal court allows for your services
before it; and
o
out-of-pocket expenses you incur or expect to
incur, for example, the cost of getting evidence.
Our approval is not needed for such expenses.
If you
are not an attorney,
you must collect the approved
fee from t he claimant.
If you are an attorney, we usually withhold 25 percent of
any past-due benefits that result from a favorably decided
retirement, survivors, disability insurance, or black lung
claim. Once we approve a fee, we pay you all or part of
the fee from the funds withheld. We will also charge you
the assessment required by section 206(d) of the Social
Security Act. You cannot charge or collect this expense
from the claimant. You must collect from the claimant:
o the rest he or she owes - if the amount of the fee is more than the
amount of money we withheld and paid you
for the claimant, and any amount you held for
the claimant in a trust or escrow account.
o all of the fee he or she owes - if we did not withhold past-due benefits, for example, because the benefits are
supplemental security income or there are
no past-due benefits; or if we withheld,
but later paid the money to the claimant
because you did not either ask for our
approval until after 60 days of the date of
the notice of award or tell us on time that
you planned to ask for a fee.
Conflict Of Interest And Penalties
For improper acts, you can be suspended or disqualified
from representing anyone before the Social Security
Administration. You also can face criminal prosecution.
Improper acts include: o If you are or were an officer or employee of the
United States, providing services as a representative
in certain claims against and other matters affecting the Federal government.
o Knowingly and willingly furnishing false information. o Charging or collecting an unauthorized fee or too
much for services provided in any claim, including
services before a court which made a favorable decision.
References o 18 U.S.C. §§ 203, 205, and 207; 30 U.S.C. § 923(b);
and 42 U.S.C. §§ 406(a), 1320a-6, and 1383(d)(2)
o 20 CFR §§ 404.1700 et. seq., 410.684 et. seq., and
416.1500 et. seq.
o
Social Security Rulings 88-10c (C.E. 1988), 85-3
(C.E. 1985), 83-27 (C.E. 1983), and 82-39 (C.E. 1982)
Form SSA-1696-U4 (4-2002) EF (4-2002)
Social Security Administration Form Approved
Please read the back of the last copy before you complete this form. OMB No. 0960-0527
Name (Claimant) (Print or Type)
Wage Earner (If Different)
Social Security Number
Social Security Number
Part I APPOINTMENT OF REPRESENTATIVE
I appoint this person, ,
(Name and Address)
to act as my representative in connection with my claim(s) or asserted right(s) under:
Title II Title XVI Title IV FMSHA Title XVIII Title VIII
(RSDI) (SSI) (Black Lung) (Medicare Coverage) (SVB)
This person may, entirely in my place, make any request or give any notice; give or draw out evidence or
information; get information; and receive any notice in connection with my pending claim(s) or asserted
right(s).
I am appointing, or I now have, more than one representative. My main representative is .
(Name of Principal Representative)
Signature (Claimant)
Telephone Number (with Area Code) Address
Date
Part II ACCEPTANCE OF APPOINTMENT
I, , hereby accept the above appointment. I certify that I
have not been suspended or prohibited from practice before the Social Security Administration; that I am
not disqualified from representing the claimant as a current or former officer or employee of the United States; and that I will not charge or collect any fee for the representation, even if a third party will pay
the fee, unless it has been approved in accordance with the laws and rules referred to on the reverse side
of the representative's copy of this form. If I decide not to charge or collect a fee for the representation, I will notify the Social Security Administration. (Completion of Part III satisfies this requirement.)
I am an attorney. I am not an attorney.
(Check one.)
Signature (Representative) Address
Telephone Number (with Area Code) Date Fax Number (with Area Code)
Part III (Optional)
WAIVER OF FEE
I waive my right to charge and collect a fee under sections 206 and 1631(d)(2) of the Social Security Act. I release my client (the claimant) from any obligations, contractual or otherwise, which may be owed to me for services I have provided in connection with my client's claim(s) or asserted right(s).
Signature (Representative) Date
Part IV (Optional)
ATTORNEY'S WAIVER OF DIRECT PAYMENT
I waive only my right to direct payment of a fee from the withheld past-due retirement, survivors,
disability insurance or black lung benefits of my client (the claimant). I do not waive my right to request fee approval and to collect a fee directly from my client or a third party.
Signature (Attorney Representative) Date
Form SSA-1696-U4 (4-2002) EF (4-2002) (See Important Information on Reverse)
OHA COPY
Destroy Prior Editions
COMPLETING THIS FORM TO APPOINT A REPRESENTATIVE
Choosing To Be Represented
You can choose to have a representative help you when you do business with Social Security. We will work with your
representative, just as we would with you. It is important that
you select a qualified person because, once appointed, your
representative may act for you in most Social Security
matters. We give more information, and examples of what a
representative may do, on the back of the "Claimant's Copy"
of this form.
Paperwork and Privacy Act Notice
The Social Security Administration will recognize someone
else as your representative if you sign a written notice
appointing that person and, if he or she is not an attorney,
that person signs the notice agreeing to be your
representative. (You can read more about this in our
regulations: 20 CFR §§ 404.1707, 410.684, and 416.1507.)
Giving the information this form requests is voluntary.
Without it though, we may not work with the person you
choose to represent you.
How To Complete This Form
Please print or type. At the top, show your full name and
your Social Security number. If your claim is based on
another person's work and earnings, also show the ''wage
earner's'' name and Social Security number. If you appoint
more than one person, you may want to complete a form for each of them.
Part I Appointment of Representative
Give the name and address of the person(s) you are appointing. You may appoint an attorney or any other qualified person to represent you. You also may appoint more
than one person, but see ''What Your Representative(s) May
Charge'' on the back of the ''Claimant's Copy'' of this form. You can appoint one or more persons
in a firm, corporation,
or other organization as your representative(s), but you may
not appoint a law firm, legal aid group, corporation, or
organization
itself.
Check the block(s) showing the program(s) under which
you have a claim. You may check more than one block. Check: o Title Il (RSDI), if your claim concerns retirement,
survivors, or disability insurance benefits.
o
Title XVI (SSI), if your claim concerns
supplemental security income.
o
Title IV FMSHA (Black Lung), if your claim
concerns black lung benefits under the Federal
Mine Safety and Health Act.
o
Title XVIII (Medicare Coverage), if your claim
concerns entitlement to Medicare or enrollment in the Supplementary Medical Insurance (SMI) plan.
If you will have more than one representative, check the
block and give the name of the person you want to be the main representative. How To Complete This Form, continued
Sign your name, but print or type your address, your area
code and telephone number, and the date.
Part II Acceptance of Appointment
Each person you appoint (named in part I) completes this
part, preferably in all cases. If the person is not an attorney, he or she must
give his or her name, state that
he or she accepts the appointment, and sign the form. Part III (Optional) Waiver of Fee
Your representative may complete this part if he or she
will not charge any fee for the services provided in this
claim. If you appoint a second representative or
co-counsel who also will not charge a fee, he or she also
should sign this part or give us a separate, written waiver statement.
Part IV (Optional) Attorney's Waiver of
Direct Payment
Your representative may complete this part if he or she is
an attorney who does not want direct payment of all or
part of the approved fee from past-due retirement,
survivors, disability insurance, or black lung benefits withheld.
This information collection meets the clearance
requirements of 44 U.S.C. § 3507, as amended by section 2 of the Paperwork
Reduction Act of 1995
. You are not
required to answer these questions unless we display a valid
Office of Management and Budget control number. We
estimate that it will take you about 10 minutes to read the instructions, gather the necessary facts, and answer the questions.
References o 18 U.S.C. §§ 203, 205, and 207; 30 U.S.C. § 923(b);
and 42 U.S.C. §§ 406(a), 1320a-6, and 1383(d)(2)
o 20 CFR §§ 404.1700 et. seq., 410.684 et. seq., and
416.1500 et. seq.
o
Social Security Rulings 88-10c (C.E. 1988), 85-3
(C.E. 1985), 83-27 (C.E. 1983), and 82-39 (C.E. 1982)
Form SSA-1696-U4 (4-2002) EF (4-2002)