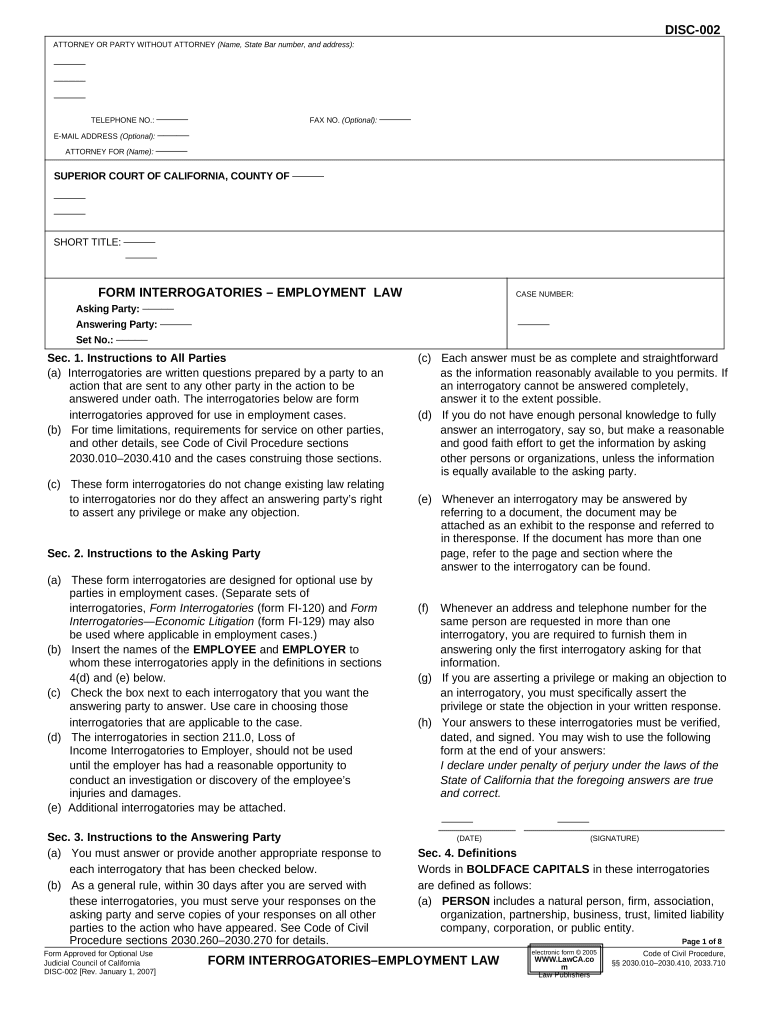
DISC-002
ATTORNEY OR PARTY WITHOUT ATTORNEY (Name, State Bar number, and address):
–––––
–––––
–––––
TELEPHONE NO.: ––––– FAX NO. (Optional): –––––
E-MAIL ADDRESS (Optional): –––––
ATTORNEY FOR (Name): –––––
SUPERIOR COURT OF CALIFORNIA, COUNTY OF –––––
–––––
–––––
SHORT TITLE: –––––
–––––
FORM INTERROGATORIES – EMPLOYMENT LAW CASE NUMBER:
Asking Party: –––––
Answering Party: ––––– –––––
Set No.: –––––
Sec. 1. Instructions to All Parties (c) Each answer must be as complete and straightforward
(a) Interrogatories are written questions prepared by a party to an as the information reasonably available to you permits. If
action that are sent to any other party in the action to be an interrogatory cannot be answered completely,
answered under oath. The interrogatories below are form answer it to the extent possible.
interrogatories approved for use in employment cases. (d) If you do not have enough personal knowledge to fully
(b) For time limitations, requirements for service on other parties, answer an interrogatory, say so, but make a reasonable
and other details, see Code of Civil Procedure sections and good faith effort to get the information by asking
2030.010–2030.410 and the cases construing those sections. other persons or organizations, unless the information
is equally available to the asking party.
(c) These form interrogatories do not change existing law relating
to interrogatories nor do they affect an answering party’s right (e) Whenever an interrogatory may be answered by
to assert any privilege or make any objection. referring to a document, the document may be
attached as an exhibit to the response and referred to
in theresponse. If the document has more than one
Sec. 2. Instructions to the Asking Party page, refer to the page and section where the
answer to the interrogatory can be found.
(a) These form interrogatories are designed for optional use by
parties in employment cases. (Separate sets of
interrogatories, Form Interrogatories (form FI-120) and Form (f) Whenever an address and telephone number for the
Interrogatories—Economic Litigation (form FI-129) may also same person are requested in more than one
be used where applicable in employment cases.) interrogatory, you are required to furnish them in
(b) Insert the names of the EMPLOYEE and EMPLOYER to answering only the first interrogatory asking for that
whom these interrogatories apply in the definitions in sections information.
4(d) and (e) below. (g) If you are asserting a privilege or making an objection to
(c) Check the box next to each interrogatory that you want the an interrogatory, you must specifically assert the
answering party to answer. Use care in choosing those privilege or state the objection in your written response.
interrogatories that are applicable to the case. (h) Your answers to these interrogatories must be verified,
(d) The interrogatories in section 211.0, Loss of dated, and signed. You may wish to use the following
Income Interrogatories to Employer, should not be used form at the end of your answers:
until the employer has had a reasonable opportunity to I declare under penalty of perjury under the laws of the
conduct an investigation or discovery of the employee’s State of California that the foregoing answers are true
injuries and damages. and correct.
(e) Additional interrogatories may be attached.
––––– –––––
Sec. 3. Instructions to the Answering Party (DATE) (SIGNATURE)
(a) You must answer or provide another appropriate response to Sec. 4. Definitions
each interrogatory that has been checked below. Words in BOLDFACE CAPITALS in these interrogatories
(b) As a general rule, within 30 days after you are served with are defined as follows:
these interrogatories, you must serve your responses on the (a) PERSON includes a natural person, firm, association,
asking party and serve copies of your responses on all other organization, partnership, business, trust, limited liability
parties to the action who have appeared. See Code of Civil company, corporation, or public entity.
Procedure sections 2030.260–2030.270 for details. Page 1 of 8
Form Approved for Optional Use Code of Civil Procedure,
Judicial Council of California §§ 2030.010–2030.410, 2033.710
DISC-002 [Rev. January 1, 2007] FORM INTERROGATORIES–EMPLOYMENT LAW electronic form ã 2005
WWW.LawCA.co
m
Law Publishers
DISC-002
(b) YOU OR ANYONE ACTING ON YOUR BEHALF includes Sec. 5. Interrogatories
you, your agents, your employees, your insurance The following interrogatories for employment law cases have
companies, their agents, their employees, your attorneys, been approved by the Judicial Council under Code of Civil
your accountants, your investigators, and anyone else acting Procedure section 2033.710:
on your behalf. CONTENTS
(c) EMPLOYMENT means a relationship in which an 200.0 Contract Formation
EMPLOYEE provides services requested by or on behalf of 201.0 Adverse Employment Action
an EMPLOYER , other than an independent contractor 202.0 Discrimination Interrogatories to Employee
relationship. 203.0 Harassment Interrogatories to Employee
(d) EMPLOYEE means a PERSON who provides services in an 204.0 Disability Discrimination
EMPLOYMENT relationship and who is a party to this lawsuit. 205.0 Discharge in Violation of Public Policy
For purposes of these interrogatories, EMPLOYEE refers to 206.0 Defamation
(insert name): ––––– 207.0 Internal Complaints
––––– 208.0 Governmental Complaints
––––– 209.0 Other Employment Claims by Employee or Against
(If no name is inserted, EMPLOYEE means all such Employer
PERSONS .) 210.0 Loss of income Interrogatories to Employee
(e) EMPLOYER means a PERSON who employs an 211.0 Loss of income Interrogatories to Employer
EMPLOYEE to provide services in an EMPLOYMENT 212.0 Physical, Mental, or Emotional Injuries—
relationship and who is a party to this lawsuit. For purposes of Interrogatories to Employee
these interrogatories, EMPLOYER refers to (insert name): 213.0 Other Damages Interrogatories to Employee
––––– 214.0 Insurance
––––– 215.0 Investigation
(If no name is inserted, EMPLOYER means all such 216.0 Denials and Special or Affirmative Defenses
PERSONS .) 217.0 Response to Request for Admissions
(f) ADVERSE EMPLOYMENT ACTION means any
TERMINATION , suspension, demotion, reprimand, loss of 200.0 Contract Formation
pay, failure or refusal to hire, failure or refusal to promote, or
other action or failure to act that adversely affects the 200.1 Do you contend that the EMPLOYMENT
EMPLOYEE’S rights or interests and which is alleged in the relationship was at “at will”? If so:
PLEADINGS . (a) state all facts upon which you base this
(g) TERMINATION means the actual or constructive termination contention;
of employment and includes a discharge, firing, layoff, (b) state the name, ADDRESS, and telephone
resignation, or completion of the term of the employment number of each PERSON who has knowledge
agreement. of those facts; and
(h) PUBLISH means to communicate orally or in writing to (c) identify all DOCUMENTS that support your
anyone other than the plaintiff. This includes communications contention.
by one of the defendant’s employees to others. (Kelly v.
General Telephone Co. (1982) 136 Cal.App.3d 278, 284.) 200.2 Do you contend that the EMPLOYMENT
(i) PLEADINGS means the original or most recent amended relationship was not “at will”? If so:
version of any complaint, answer, cross-complaint, or answer (a) state all facts upon which you base this
to cross-complaint. contention;
(b) state the name, ADDRESS , and telephone
(j) BENEFIT means any benefit from an EMPLOYER, including
an “employee welfare benefit plan” or employee pension number of each PERSON who has knowledge
benefit plan” within the meaning of Title 29 United States of those facts; and
Code section 1002(1) or (2) or ERISA. (c) identify all DOCUMENTS that support
your contention.
(k) HEALTH CARE PROVIDER includes any PERSON
referred to in Code of Civil Procedure section 667.7(e)(3).
200.3 Do you contend that the EMPLOYMENT
(l) DOCUMENT means a writing, as defined in Evidence Code relationship was governed by any
section 250, and includes the original or a copy of agreement—written, oral, or implied? If so:
handwriting, typewriting, printing, photostats, photographs, (a) state all facts upon which you base this
electronically stored information, and every other means of contention;
recording upon any tangible thing and form of communicating (b) state the name, ADDRESS, and telephone
or representation, including letters, words, pictures, sounds, number of each PERSON who has knowledge
or symbols, or combinations of them. of those facts; and
(m) ADDRESS means the street address, including the city, state, (c) identify all DOCUMENTS that support your
and zip code. contention.
Page 2 of 8
FI- DISC-002 [Rev. January 1, 2007] FORM INTERROGATORIES–EMPLOYMENT LAW
DISC-002
200.4 Was any part of the parties’ EMPLOYMENT 201.2 Are there any facts that would support the
relationship governed in whole or in part by any EMPLOYEE’S TERMINATION that were first
written rules, guidelines, policies, or procedures discovered after the TERMINATION ? If so:
established by the EMPLOYER ? If so, for each (a) state the specific facts;
DOCUMENT containing the written rules, (b) state when and how EMPLOYER first learned of
guidelines, policies, or procedures: each specific fact;
(a) state the date and title of the DOCUMENT and (c) state the name, ADDRESS , and telephone number of
a general description of its contents; each PERSON who has knowledge of the specific
(b) state the manner in which the DOCUMENT was facts; and
communicated to employees; and (d) identify all DOCUMENTS that evidence these specific
(c) state the manner, if any, in which employees facts.
acknowledged either receipt of the DOCUMENT
or knowledge of its contents. 201.3 Were there any other ADVERSE EMPLOYMENT
ACTIONS, including (the asking party should list the
200.5 Was any part of the parties’ EMPLOYMENT ADVERSE EMPLOYMENT ACTIONS ):
relationship covered by one or more collective –––––
bargaining agreements or memorandums of understanding –––––
between the EMPLOYER (or an association of employers) –––––
and any labor union or employee association? If so, for each –––––
collective bargaining agreement or memorandum of –––––
understanding, state:
(a) the names and ADDRESSES of the parties to the If so, for each action, provide the following:
collective bargaining agreement or memorandum of (a) all reasons for each ADVERSE EMPLOYMENT
understanding; ACTION ;
(b) the beginning and ending dates, if applicable, of the (b) the name, ADDRESS , and telephone number of
collective bargaining agreement or memorandum of each PERSON who participated in making each
ADVERSE EMPLOYMENT ACTION decision;
understanding; and
(c) which parts of the collective bargaining agreement or (c) the name, ADDRESS, and telephone number
memorandum of understanding, if any, govern (1) of each PERSON who provided any information
any dispute or claim referred to in the PLEADINGS relied upon in making each ADVERSE
EMPLOYMENT ACTION decision;
and
and (2) the rules or procedures for resolving any
dispute or claim referred to in the PLEADINGS . (d) the identity of all DOCUMENTS relied upon
in making each ADVERSE EMPLOYMENT
200.6 Do you contend that the EMPLOYEE and the ACTION decision.
EMPLOYER were in a business relationship other
than an EMPLOYMENT relationship? If so, for each 201.4 Was the TERMINATION or any other
relationship: ADVERSE EMPLOYMENT ACTIONS referred to in
(a) state the names of the parties to the relationship; Interrogatories 201.1 through 201.3 based in whole or in
(b) identify the relationship; and part on the EMPLOYEE'S job performance? If so, for each
(c) state all facts upon which you base your contention action:
that the parties were in a relationship other than an (a) identify the ADVERSE EMPLOYMENT ACTION ;
EMPLOYMENT relationship. (b) identify the EMPLOYEE'S specific job
performance that played a role in that
ADVERSE EMPLOYMENT ACTION ;
201.0 Adverse Employment Action (c) identify any rules, guidelines, policies, or
201.1 Was the EMPLOYEE involved in a TERMINATION ? procedures that were used to evaluate the
If so: EMPLOYEE’S specific job performance;
(a) state all reasons for the EMPLOYEE’S (d) state the names, ADDRESSES , and telephone
TERMINATION ; numbers of all PERSONS who had responsibility for
(b) state the name, ADDRESS , and telephone number of evaluating the specific job performance of the
each PERSON who participated in the EMPLOYEE ;
TERMINATION decision; (e) state the names, ADDRESSES, and telephone
(c) state the name, ADDRESS , and telephone number of numbers of all PERSONS who have knowledge of the
each PERSON who provided any information relied EMPLOYEE'S specific job performance that played a
upon in the TERMINATION decision; and role in that ADVERSE EMPLOYMENT ACTION ; and
(d) identify all DOCUMENTS relied upon in the (f) describe all warnings given with respect to the
TERMINATION decision. EMPLOYEE’S specific job performance.
Page 3 of 8
DISC-002 [Rev. January 1, 2007] FORM INTERROGATORIES–EMPLOYMENT LAW
DISC-002
201.5 Was any PERSON hired to replace the (c) identify each characteristic (for example, gender,
EMPLOYEE after the EMPLOYEE’S race, age, etc.) on which you base your claim of
TERMINATION or demotion? If so, state the harassment;
PERSON'S name, job title, qualifications, (d) state all facts upon which you base your
ADDRESS and telephone number, and the contention that you were unlawfully harassed;
date the PERSON was hired. (e) state the name, ADDRESS , and telephone
number of each PERSON with knowledge
of those facts; and
201.6 Has any PERSON performed any of the (f) identify all DOCUMENTS evidencing those facts.
EMPLOYEE’S former job duties after the
EMPLOYEE’S TERMINATION or demotion? If so: 204.0 Disability Discrimination
(a) state the PERSON’S name, job title,
ADDRESS, and telephone number; 204.1 Name and describe each disability alleged in the
(b) identify the duties; and PLEADINGS .
(c) state the date on which the PERSON started to
perform the duties. 204.2 Does the EMPLOYEE allege any injury or
illness that arose out of or in the course of
EMPLOYMENT ?
201.7 If the ADVERSE EMPLOYMENT ACTION involved If so, state:
the failure or refusal to select the EMPLOYEE (for (a) the nature of such injury or illness;
example, for hire, promotion, transfer, or training), was (b) how such injury or illness occurred;
any other PERSON selected instead? If so, for each (c) the date on which such injury or illness
ADVERSE EMPLOYMENT ACTION, state the name, occurred;
ADDRESS , and telephone number of each PERSON (d) whether EMPLOYEE has filed a workers’
selected; the date the PERSON was selected; and the compensation claim. If so, state the date and
reason the PERSON was selected instead of the outcome of the claim; and
EMPLOYEE . (e) whether EMPLOYEE has filed or applied
for disability benefits of any type. If so, state the
202.0 Discrimination—Interrogatories to Employee date, identify the nature of the benefits
applied for, and the outcome of any such
application.
202.1 Do you contend that any ADVERSE
EMPLOYMENT ACTIONS against you were 204.3 Were there any communications between the
discriminatory? If so: EMPLOYEE (or the EMPLOYEE’S HEALTH CARE
(a) identify each ADVERSE EMPLOYMENT PROVIDER) and the EMPLOYER about the type or
ACTION that involved unlawful discrimination; extent of any disability of EMPLOYEE ? If so:
(b) identify each characteristic (for example, gender, (a) state the name, ADDRESS , and telephone
race, age, etc.) on which you base your claim or number of each person who made or received
claims of discrimination; the communications;
(c) state all facts upon which you base each claim (b) state the name, ADDRESS , and telephone
of discrimination; number of each PERSON who witnessed the
(d) state the name, ADDRESS , and telephone number of communications;
each PERSON with knowledge of those facts; and (c) describe the date and substance of the
(e) identify all DOCUMENTS evidencing those facts. communications; and
(d) identify each DOCUMENT that refers to the
202.2 State all facts upon which you base your contention communications.
that you were qualified to perform any job which you
contend was denied to you on account of unlawful 204.4 Did the EMPLOYER have any information
discrimination. about the type, existence, or extent of any disability of
EMPLOYEE other than from communications with the
203.0 Harassment—Interrogatories to Employee EMPLOYEE or the EMPLOYEE’S HEALTH CARE
PROVIDER ? If so, state the sources and substance of
203.1 Do you contend that you were unlawfully harassed in that information and the name, ADDRESS, and
your employment? If so: telephone number of each PERSON who provided or
(a) state the name, ADDRESS, telephone number, and received the information.
employment position of each PERSON whom you
contend harassed you; 204.5 Did the EMPLOYEE need any
(b) for each PERSON whom you contend harassed you, accommodation to perform any function of the
describe the harassment; EMPLOYEE’S job position or need a transfer
to another position as an accommodation? If
so,
describe the accommodations needed. Page 4 of 8
DISC-002 [Rev. January 1, 2007] FORM INTERROGATORIES–EMPLOYMENT LAW
DISC-002
204.6 Were there any communications between the (d) state whether, at the time the statement was
EMPLOYEE (or the EMPLOYEE’S HEALTH CARE PUBLISHED , the PERSON who PUBLISHED the
PROVIDER ) and the EMPLOYER about any possible statement believed it to be true; and
accommodation of EMPLOYEE ? If so, for each (e) state all facts upon which the PERSON who
communication: published the statement based the belief that it was
(a) state the name, ADDRESS , and telephone true.
number of each PERSON who made or
received the communication; 206.2 State the name and ADDRESS of each agent or
(b) state the name, ADDRESS , and telephone employee of the EMPLOYER who responded to any
number of each PERSON who witnessed the inquiries regarding the EMPLOYEE after the
communication; EMPLOYEE’S TERMINATION .
(c) describe the date and substance of the
communication; and 206.3 State the name and ADDRESS of the recipient
(d) identify each DOCUMENT that refers to the and the substance of each post- TERMINATION
communication. statement PUBLISHED about EMPLOYEE by
any agent or employee of EMPLOYER .
204.7 What did the EMPLOYER consider doing to
accommodate the EMPLOYEE ? For each 207.0 Internal Complaints
accommodation considered:
(a) describe the accommodation considered; 207.1 Were there any internal written policies or
(b) state whether the accommodation was offered to the regulations of the EMPLOYER that apply to the making
EMPLOYEE ; of a complaint of the type that is the subject matter of
(c) state the EMPLOYEE’S response; or this lawsuit? If so:
(d) if the accommodation was not offered, state all the (a) state the title and date of each DOCUMENT
reasons why this decision was made; containing the policies or regulations and a
(e) state the name, ADDRESS , and telephone number of general description of the DOCUMENT’S
each PERSON who on behalf of EMPLOYER made contents;
any decision about what accommodations, if any, to (b) state the manner in which the DOCUMENT was
make for the EMPLOYEE ; and communicated to EMPLOYEES ;
(f) state the name, ADDRESS , and telephone number of (c) state the manner, if any, in which EMPLOYEES
each PERSON who on behalf of the EMPLOYER acknowledged receipt of the DOCUMENT or
made or received any communications about what knowledge of its contents, or both;
accommodations, if any, to make for the (d) state, if you contend that the EMPLOYEE failed
EMPLOYEE . to use any available internal complaint
205.0 Discharge in Violation of Public Policy procedures, all facts that support
that contention; and
205.1 Do you contend that the EMPLOYER took any (e) state, if you contend that the EMPLOYEE’S
ADVERSE EMPLOYMENT ACTION against you in failure to use internal complaint procedures was
violation of public policy? If so: excused, all facts why the EMPLOYEE’S use of
(a) identify the constitutional provision, statute, the procedures was excused.
regulation, or other source of the public policy that
you contend was violated; and 207.2 Did the EMPLOYEE complain to the
(b) state all facts upon which you base your contention EMPLOYER about any of the unlawful conduct
that the EMPLOYER violated public policy. alleged in the PLEADINGS ? If so, for
each complaint:
206.0 Defamation (a) state the date of the complaint;
(b) state the nature of the complaint;
206.1 Did the EMPLOYER'S agents or employees (c) state the name and ADDRESS of each
PUBLISH any of the allegedly defamatory statements PERSON to whom the complaint was made;
identified in the PLEADINGS ? If so, for each (d) state the name, ADDRESS , telephone number,
statement: and job title of each PERSON who investigated
(a) identify the PUBLISHED statement; the complaint;
(b) state the name, ADDRESS, telephone number, and (e) state the name, ADDRESS , telephone number,
job title of each person who PUBLISHED the and job title of each PERSON who participated
statement; in making decisions about how to conduct the
(c) state the name, ADDRESS , and telephone number of investigation;
each person to whom the statement was
PUBLISHED ;
Page 5 of 8
DISC-002 [Rev. January 1, 2007] FORM INTERROGATORIES–EMPLOYMENT LAW
DISC-002
(f) state the name, ADDRESS, telephone number, (d) state the name, ADDRESS , telephone number, and
and job title of each PERSON who was job title of each PERSON who was interviewed or
interviewed or who provided an oral or written who provided an oral or written statement as part of
statement as part of the investigation of the complaint; the investigation.
(g) state the nature and date of any action taken in 209.0 Other Employment Claims by Employee or
response to the complaint; Against Employer
(h) state whether the EMPLOYEE who made the
complaint was made aware of the actions taken 209.1 Except for this action, in the past 10 years has
by the EMPLOYER in response to the the EMPLOYEE filed a civil action against any
complaint, and, if so, state how and when; employer regarding the EMPLOYEE’S employment? If
(i) identify all DOCUMENTS relating to the so, for each civil action:
complaint, the investigation, and any action (a) state the name, ADDRESS, and telephone
taken in response to the complaint; and number of each employer against whom the
(j) state the name, ADDRESS , and telephone action was filed;
number of each PERSON who has knowledge (b) state the court, names of the parties, and case
of the EMPLOYEE’S complaint or the number of the civil action;
EMPLOYER'S response to the complaint. (c) state the name, ADDRESS , and
telephone number of any attorney
representing the
208.0 Governmental Complaints EMPLOYEE ; and
(d) state whether the action has been resolved
208.1 Did the EMPLOYEE file a claim, complaint, or charge or is pending.
with any governmental agency that involved any of the
material allegations made in the PLEADINGS ? If so, for 209.2 Except for this action, in the past 10 years has
each claim, complaint, or charge: any employee filed a civil action against the
(a) state the date on which it was filed; EMPLOYER regarding his or her employment?
(b) state the name and ADDRESS of the agency with If so, for each civil action:
which it was filed; (a) state the name, ADDRESS , and telephone
(c) state the number assigned to the claim, complaint, or number of each employee who filed the action;
charge by the agency; (b) state the court, names of the parties, and case
(d) state the nature of each claim, complaint, or charge number of the civil action;
made; (c) state the name, ADDRESS , and telephone
(e) state the date on which the EMPLOYER was number of any attorney representing the
notified of the claim, complaint, or charge; EMPLOYER ; and
(f) state the name, ADDRESS , and telephone number of (d) state whether the action has been resolved or
all PERSONS within the governmental agency with is pending.
whom the EMPLOYER has had any contact or
communication regarding the claim, complaint, or 210.0 Loss of Income—Interrogatories to Employee
charge;
(g) state whether a right to sue notice was issued and, if 210.1 Do you attribute any loss of income, benefits,
so, when; and or earning capacity to any ADVERSE
(h) state whether any findings or conclusions regarding EMPLOYMENT ACTION? (If your answer is “no,” do
the complaint or charge have been made, and, if so, not answer Interrogatories 210.2 through 210.6.)
the date and description of the agency’s findings or
conclusions. 210.2 State the total amount of income, benefits,
or earning capacity you have lost to date and how
the amount was calculated.
208.2 Did the EMPLOYER respond to any claim,
complaint, or charge identified in Interrogatory 208.1? If so,
for each claim, complaint, or charge: 210.3 Will you lose income, benefits, or earning
(a) state the nature and date of any investigation done or capacity in the future as a result of any ADVERSE
any other action taken by the EMPLOYER in EMPLOYMENT ACTION ? If so, state the total amount
response to the claim, complaint, or charge: of income, benefits, or earning capacity you expect to
(b) state the name, ADDRESS , telephone number, and lose, and how the amount was calculated.
job title of each person who investigated the claim,
complaint, or charge; 210.4 Have you attempted to minimize the amount of
(c) state the name, ADDRESS , telephone number, and your lost income? If so, describe how; if not,
job title of each PERSON who participated in making explain why not.
decisions about how to conduct the investigation; and
Page 6 of 8
DISC-002 [Rev. January 1, 2007] FORM INTERROGATORIES–EMPLOYMENT LAW
DISC-002
210.5 Have you purchased any benefits to replace 212.0 Physical, Mental, or Emotional Injuries—
any benefits to which you would have been entitled if Interrogatories to Employee
the ADVERSE EMPLOYMENT ACTION had not
occurred? If so, state the cost for each benefit 212.1 Do you attribute any physical, mental, or emotional
purchased. injuries to the ADVERSE EMPLOYMENT ACTION ? (If
your answer is “no,” do not answer Interrogatories
212.2
210.6 Have you obtained other employment since any through 212.7.)
ADVERSE EMPLOYMENT ACTION ? If so, for each new
employment: 212.2 Identify each physical, mental, or emotional
(a) state when the new employment commenced; injury that you attribute to the ADVERSE
(b) state the hourly rate or monthly salary for the EMPLOYMENT ACTION and the area of your body
new employment; and affected.
(c) state the benefits available from the new
employment. 212.3 Do you still have any complaints of physical,
mental, or emotional injuries that you attribute to the
211.0 Loss of Income—Interrogatories to Employer ADVERSE EMPLOYMENT ACTION ? If so, for each
[See instruction 2(d).] complaint state:
(a) a description of the injury;
211.1 Identify each type of BENEFIT to which the (b) whether the complaint is subsiding, remaining
EMPLOYEE would have been entitled, from the date the same, or becoming worse; and
of the ADVERSE EMPLOYMENT ACTION to the (c) the frequency and duration.
present, if the ADVERSE EMPLOYMENT ACTION
had not happened and the EMPLOYEE had 212.4 Did you receive any consultation or examination
remained in the same job position. For each type of (except from expert witnesses covered by Code of Civil
benefit, state the amount the EMPLOYER would Procedure section 2034) or treatment from a HEALTH
have paid to provide the benefit for the EMPLOYEE CARE PROVIDER for any injury you attribute to the
during this time period and the value of the BENEFIT ADVERSE EMPLOYMENT ACTION ? If so, for each
to the EMPLOYEE . HEALTH CARE PROVIDER state:
(a) the name, ADDRESS, and telephone number;
211.2 Do you contend that the EMPLOYEE has not made (b) the type of consultation, examination, or
reasonable efforts to minimize the amount of the treatment provided;
EMPLOYEE’S lost income? If so: (c) the dates you received consultation,
(a) describe what more EMPLOYEE should have done; examination, or treatment; and
(b) state the names, ADDRESSES , and telephone (d) the charges to date.
numbers of all PERSONS who have knowledge of
the facts that support your contention; and 212.5 Have you taken any medication, prescribed or
(c) identify all DOCUMENTS that support your not, as a result of injuries that you attribute to the
contention and state the name, ADDRESS , and ADVERSE EMPLOYMENT ACTION ? If so, for each
telephone number of the PERSON who has each medication state:
DOCUMENT . (a) the name of the medication;
211.3 Do you contend that any of the lost income claimed (b) the name, ADDRESS and telephone number of
by the EMPLOYEE , as disclosed in discovery thus far the PERSON who prescribed or furnished it;
in this case, is unreasonable or was not caused by (c) the date prescribed or furnished;
the ADVERSE EMPLOYMENT ACTION ? If so: (d) the dates you began and stopped taking it; and
(a) state the amount of claimed lost income that you (e) the cost to date.
dispute;
(b) state all facts upon which you base your contention; 212.6 Are there any other medical services not
(c) state the names, ADDRESSES , and telephone previously listed in response to interrogatory 212.4 (for
numbers of all PERSONS who have knowledge of example, ambulance, nursing, prosthetics) that you
the facts; and received for injuries attributed to the ADVERSE
(d) identify all DOCUMENTS that support your EMPLOYMENT ACTION ? If so, for each service state:
contention and state the name, ADDRESS , and (a) the nature;
telephone number of the PERSON who has each (b) the date;
DOCUMENT . (c) the cost; and
(d) the name, ADDRESS , and telephone number
of each HEALTH CARE PROVIDER .
Page 7 of 8
DISC-002 [Rev. January 1, 2007] FORM INTERROGATORIES–EMPLOYMENT LAW
DISC-
002
212.7 Has any HEALTH CARE PROVIDER advised 215.0 Investigation
that you may require future or additional treatment for
any injuries that you attribute to the ADVERSE 215.1 Have YOU OR ANYONE ACTING ON YOUR
EMPLOYMENT ACTION ? If so, for each injury state: BEHALF interviewed any individual concerning the
(a) the name and ADDRESS of each HEALTH ADVERSE EMPLOYMENT ACTION ? If so, for each
CARE PROVIDER ; individual state:
(b) the complaints for which the treatment was advised; (a) the name, ADDRESS , and telephone number of
and the individual interviewed;
(c) the nature, duration, and estimated cost of the (b) the date of the interview; and
treatment. (c) the name, ADDRESS, and telephone number of
the PERSON who conducted the interview.
213.0 Other Damages—Interrogatories to Employee
215.2 Have YOU OR ANYONE ACTING ON YOUR
213.1 Are there any other damages that you attribute to BEHALF obtained a written or recorded statement from
the ADVERSE EMPLOYMENT ACTION ? If so, for any individual concerning the ADVERSE EMPLOYMENT
each item of damage state: ACTION? If so, for each statement state:
(a) the nature; (a) the name, ADDRESS , and telephone number of
(b) the date it occurred; the individual from whom the statement was
(c) the amount; and obtained;
(d) the name, ADDRESS , and telephone number of (b) the name, ADDRESS , and telephone number of
each PERSON who has knowledge of the the individual who obtained the statement;
nature or amount of the damage. (c) the date the statement was obtained; and
(d) the name, ADDRESS , and telephone number of
213.2 Do any DOCUMENTS support the existence or each PERSON who has the original statement or
amount of any item of damages claimed in Interrogatory a copy.
213.1 ? If so, identify the DOCUMENTS and state the name,
ADDRESS , and telephone number of the PERSON who 216.0 Denials and Special or Affirmative Defenses
has each DOCUMENT .
216.1 Identify each denial of a material allegation
214.0 Insurance and each special or affirmative defense in your
PLEADINGS and for each:
214.1 At the time of the ADVERSE EMPLOYMENT (a) state all facts upon which you base the denial or
ACTION , was there in effect any policy of insurance special or affirmative defense;
through which you were or might be insured in any (b) state the names, ADDRESSES , and telephone
manner for the damages, claims, or actions that have numbers of all PERSONS who have knowledge
arisen out of the ADVERSE EMPLOYMENT ACTION ? of those facts; and
If so, for each policy state: (c) identify all DOCUMENTS and all other tangible
(a) the kind of coverage; things, that support your denial or special or
(b) the name and ADDRESS of the insurance affirmative defense, and state the name,
company; ADDRESS , and telephone number of the
(c) the name, ADDRESS , and telephone number of PERSON who has each DOCUMENT .
each named insured;
(d) the policy number; 217.0 Response to Request for Admissions
(e) the limits of coverage for each type of coverage
contained in the policy; 217.1 Is your response to each request for admission
(f) whether any reservation of rights or controversy served with these interrogatories an unqualified
or coverage dispute exists between you and the admission? If not, for each response that is not an
insurance company; and unqualified admission:
(g) the name, ADDRESS , and telephone number of (a) state the number of the request;
the custodian of the policy. (b) state all facts upon which you base
your response;
214.2 Are you self-insured under any statute for the (c) state the names, ADDRESSES, and telephone
damages, claims, or actions that have arisen out of the numbers of all PERSONS who have knowledge
ADVERSE EMPLOYMENT ACTION ? If so, specify the of those facts; and
statute. (d) identify all DOCUMENTS and other tangible
things that support your response and state the
name, ADDRESS , and telephone number of the
PERSON who has each DOCUMENT or thing.
Page 8 of 8
DISC-002 [Rev. January 1, 2007] FORM INTERROGATORIES–EMPLOYMENT LAW