
Fill and Sign the Michigan Affidavit Successor Form
Useful Suggestions for Finalizing Your ‘Michigan Affidavit Successor Form’ Digitally
Are you fed up with the inconvenience of handling paperwork? Look no further than airSlate SignNow, the premier electronic signature solution for individuals and small to medium-sized businesses. Bid farewell to the lengthy routine of printing and scanning documents. With airSlate SignNow, you can effortlessly finalize and sign paperwork online. Utilize the powerful tools integrated into this user-friendly and cost-effective platform to transform your document management strategy. Whether you need to authorize forms or collect signatures, airSlate SignNow simplifies the process, needing just a few clicks.
Adhere to this comprehensive guide:
- Sign in to your account or initiate a complimentary trial with our service.
- Hit +Create to upload a file from your device, cloud storage, or our collection of templates.
- Access your ‘Michigan Affidavit Successor Form’ in the editor.
- Select Me (Fill Out Now) to set up the document on your end.
- Add and designate fillable fields for others (if necessary).
- Proceed with the Send Invite settings to solicit eSignatures from others.
- Download, print a copy, or convert it into a multi-use template.
Don’t fret if you need to work with your colleagues on your Michigan Affidavit Successor Form or send it for notarization—our platform provides you with everything you require to achieve such objectives. Register with airSlate SignNow today and enhance your document management to a new height!
FAQs
-
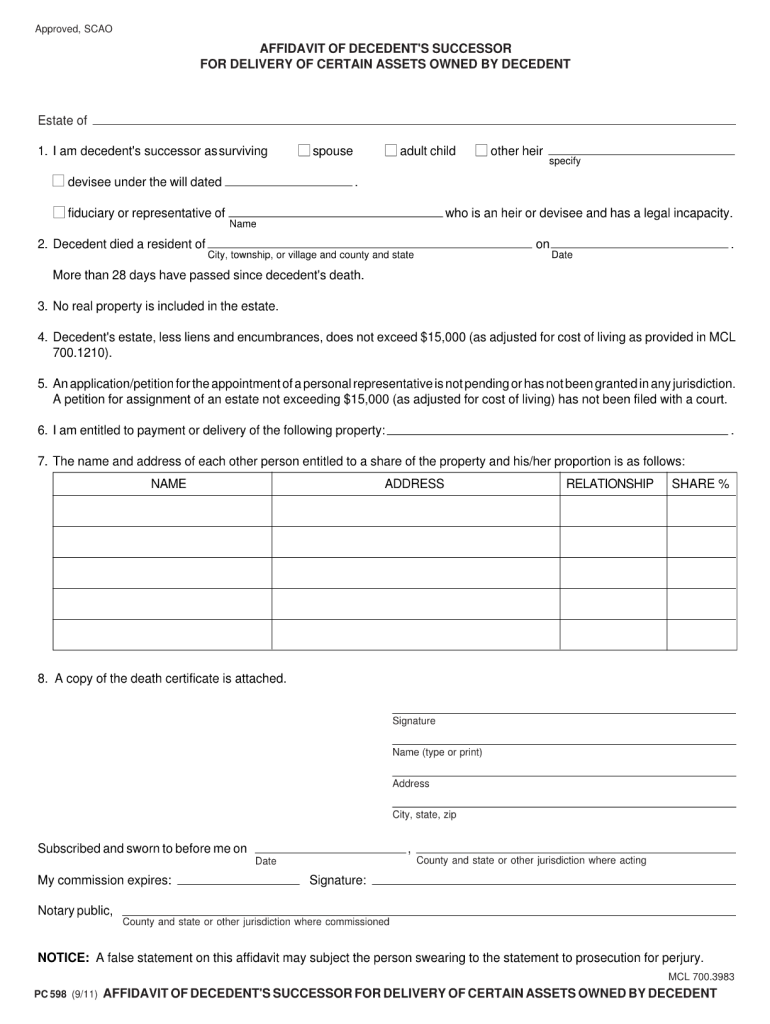
What is the Michigan Small Estate Affidavit Form Pc 598?
The Michigan Small Estate Affidavit Form Pc 598 is a legal document that allows heirs to claim assets of a deceased person without going through formal probate. This form simplifies the process for small estates, enabling beneficiaries to access funds and property more efficiently.
-
How can I fill out the Michigan Small Estate Affidavit Form Pc 598 using airSlate SignNow?
Filling out the Michigan Small Estate Affidavit Form Pc 598 with airSlate SignNow is simple. You can upload the form, fill in the necessary details, and eSign it electronically, ensuring a hassle-free experience. This digital solution streamlines the entire process, making it quick and efficient.
-
Is there a cost associated with using airSlate SignNow for the Michigan Small Estate Affidavit Form Pc 598?
Yes, airSlate SignNow offers various pricing plans that are cost-effective for users needing to complete the Michigan Small Estate Affidavit Form Pc 598. You can choose a plan that fits your budget and requirements, ensuring you get the best value for your document signing needs.
-
What are the benefits of using airSlate SignNow for the Michigan Small Estate Affidavit Form Pc 598?
Using airSlate SignNow for the Michigan Small Estate Affidavit Form Pc 598 offers numerous benefits, including fast eSigning, document tracking, and secure storage. This platform enhances efficiency and ensures that all parties involved can access and sign the document seamlessly.
-
Can I integrate airSlate SignNow with other applications for the Michigan Small Estate Affidavit Form Pc 598?
Absolutely! airSlate SignNow allows integrations with various applications, enabling you to manage your documents effectively. This means you can easily connect it with your existing software, enhancing your workflow when handling the Michigan Small Estate Affidavit Form Pc 598.
-
Is my data secure when using airSlate SignNow for the Michigan Small Estate Affidavit Form Pc 598?
Yes, airSlate SignNow prioritizes your data security. When using the platform for the Michigan Small Estate Affidavit Form Pc 598, your information is protected with advanced encryption and security measures, ensuring that your documents and personal data remain confidential.
-
Can multiple people sign the Michigan Small Estate Affidavit Form Pc 598 electronically with airSlate SignNow?
Yes, airSlate SignNow allows multiple parties to electronically sign the Michigan Small Estate Affidavit Form Pc 598. This feature facilitates collaboration among heirs and simplifies the signing process, making it convenient for everyone involved.
Find out other michigan affidavit successor form
- Close deals faster
- Improve productivity
- Delight customers
- Increase revenue
- Save time & money
- Reduce payment cycles
