
Fill and Sign the Pacificare Authorization Form
Convenient tips on preparing your ‘Pacificare Authorization Form’ online
Are you fed up with the inconvenience of dealing with paperwork? Look no further than airSlate SignNow, the premier electronic signature solution for both individuals and entities. Bid farewell to the lengthy process of printing and scanning documents. With airSlate SignNow, you can seamlessly finalize and sign papers online. Utilize the powerful features integrated into this user-friendly and cost-effective platform and transform your method of document management. Whether you need to approve forms or collect signatures, airSlate SignNow manages it all effortlessly, requiring merely a few clicks.
Follow this detailed guide:
- Sign in to your account or initiate a free trial with our service.
- Click +Create to upload a file from your device, cloud storage, or our form library.
- Access your ‘Pacificare Authorization Form’ in the editor.
- Click Me (Fill Out Now) to finalize the document on your end.
- Add and designate fillable fields for others (if necessary).
- Proceed with the Send Invite options to solicit eSignatures from others.
- Download, print your copy, or convert it into a reusable template.
No need to worry if you need to collaborate with your colleagues on your Pacificare Authorization Form or send it for notarization—our solution offers everything you require to accomplish such tasks. Sign up with airSlate SignNow today and take your document management to new heights!
FAQs
-
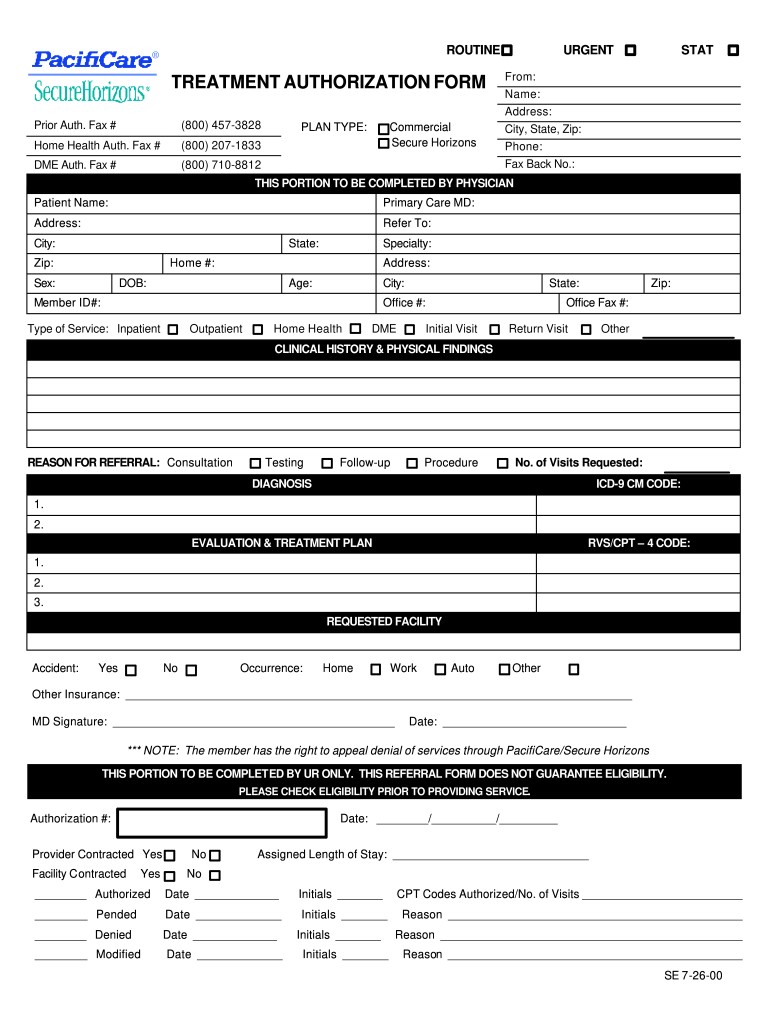
What is the Pacificare Prior Authorization Form?
The Pacificare Prior Authorization Form is a document required by Pacificare to obtain prior approval for specific medical services or medications. By using airSlate SignNow, you can easily complete and eSign the Pacificare Prior Authorization Form, streamlining the approval process for you and your healthcare provider.
-
How does airSlate SignNow help with the Pacificare Prior Authorization Form?
airSlate SignNow simplifies the completion of the Pacificare Prior Authorization Form by providing an intuitive interface for filling out and signing documents electronically. This not only saves time but also reduces the risk of errors, ensuring that your requests are processed quickly and efficiently.
-
Is there a cost associated with using airSlate SignNow for the Pacificare Prior Authorization Form?
airSlate SignNow offers a cost-effective solution for managing documents, including the Pacificare Prior Authorization Form. Our pricing plans are designed to fit various budgets, allowing you to choose the one that best suits your needs without compromising on features or functionality.
-
Can I integrate airSlate SignNow with other software for the Pacificare Prior Authorization Form?
Yes, airSlate SignNow supports seamless integrations with various software applications, enhancing your workflow for the Pacificare Prior Authorization Form. Whether you’re using healthcare management systems or CRM software, you can easily connect airSlate SignNow to streamline your document management process.
-
What are the benefits of using airSlate SignNow for the Pacificare Prior Authorization Form?
Using airSlate SignNow for the Pacificare Prior Authorization Form offers numerous benefits, including faster processing times, reduced paperwork, and enhanced security for your sensitive information. Additionally, the ability to track document status in real-time ensures that you stay updated on the progress of your authorization requests.
-
How secure is my information when using airSlate SignNow for the Pacificare Prior Authorization Form?
Security is a top priority for airSlate SignNow. When you use our services for the Pacificare Prior Authorization Form, your data is protected with industry-standard encryption and compliance with regulations, ensuring that your information remains confidential and secure throughout the signing process.
-
Can multiple users collaborate on the Pacificare Prior Authorization Form using airSlate SignNow?
Absolutely! airSlate SignNow allows for multiple users to collaborate on the Pacificare Prior Authorization Form. This feature enables healthcare providers and administrative staff to work together efficiently, ensuring that all necessary information is included and the form is submitted without delay.
Find out other pacificare authorization form
- Close deals faster
- Improve productivity
- Delight customers
- Increase revenue
- Save time & money
- Reduce payment cycles
