
Fill and Sign the Transcript Request Form Owens Community College Owens
Helpful advice on preparing your ‘Transcript Request Form Owens Community College Owens’ online
Are you fed up with the inconvenience of managing documents? Search no further than airSlate SignNow, the leading eSignature service for individuals and corporations. Bid farewell to the lengthy procedure of printing and scanning documents. With airSlate SignNow, you can effortlessly finalize and sign documents online. Utilize the powerful features embedded in this user-friendly and cost-effective platform and transform your method of document management. Whether you need to approve documents or collect eSignatures, airSlate SignNow takes care of everything seamlessly, needing just a few clicks.
Adhere to this detailed guide:
- Log into your account or sign up for a complimentary trial with our service.
- Click +Create to import a file from your device, cloud storage, or our template library.
- Access your ‘Transcript Request Form Owens Community College Owens’ in the editor.
- Click Me (Fill Out Now) to prepare the document on your end.
- Add and designate fillable fields for other participants (if needed).
- Proceed with the Send Invite options to request eSignatures from others.
- Download, print your copy, or convert it into a reusable template.
No need to worry if you need to collaborate with your colleagues on your Transcript Request Form Owens Community College Owens or submit it for notarization—our service offers everything necessary to complete such tasks. Register with airSlate SignNow today and elevate your document management to a new standard!
FAQs
-
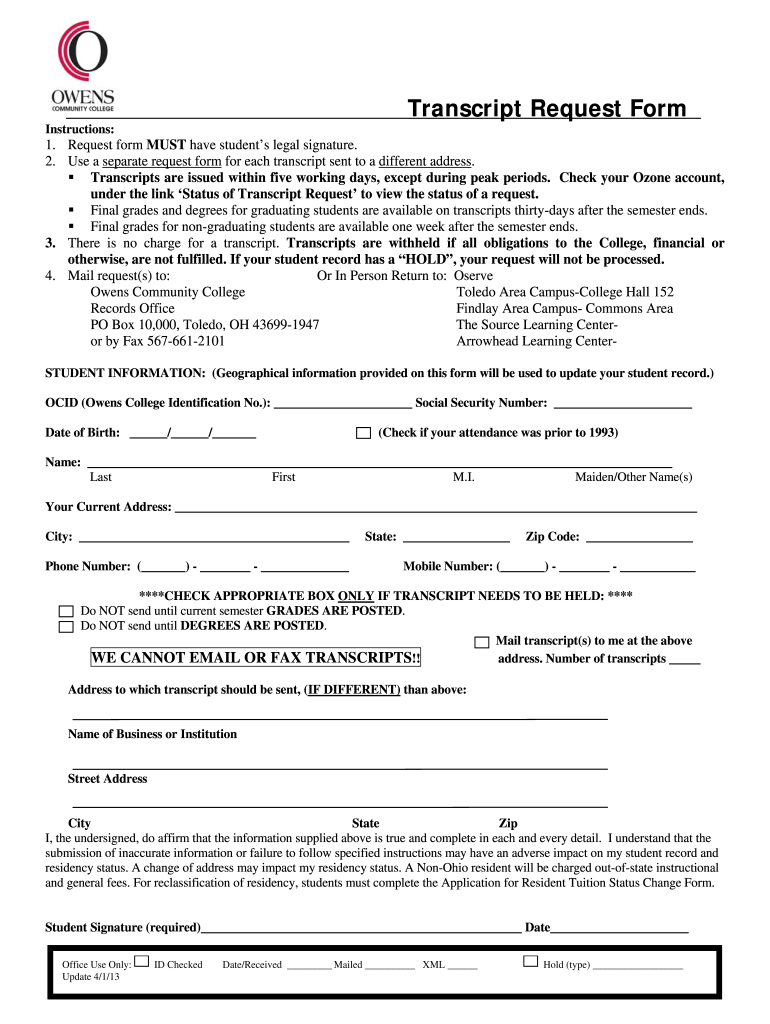
What is the Transcript Request Form Owens Community College Owens?
The Transcript Request Form Owens Community College Owens is a formal document that students and alumni can use to request their academic transcripts. This form enables you to obtain your academic records efficiently, ensuring that your educational achievements are readily available whenever needed.
-
How do I complete the Transcript Request Form Owens Community College Owens?
To complete the Transcript Request Form Owens Community College Owens, simply download the form from the college's website, fill in your details, and submit it as instructed. Make sure to provide accurate information to avoid any processing delays.
-
What are the fees associated with the Transcript Request Form Owens Community College Owens?
The fees for processing the Transcript Request Form Owens Community College Owens vary based on the type of delivery method chosen. Typically, there is a nominal fee for standard processing, with additional charges for expedited requests. Be sure to check the college’s website for the most current pricing.
-
How long does it take to process the Transcript Request Form Owens Community College Owens?
Processing time for the Transcript Request Form Owens Community College Owens can vary depending on the method of request. Generally, standard requests take about 5-7 business days, while expedited requests are processed within 1-3 business days. Always check for specific timelines on the college's site.
-
Can I submit the Transcript Request Form Owens Community College Owens online?
Yes, you can submit the Transcript Request Form Owens Community College Owens online. Many institutions now offer digital submission options, allowing for quicker processing. Check the Owens Community College website for specific instructions on how to submit your request electronically.
-
What if I have issues with the Transcript Request Form Owens Community College Owens?
If you encounter any issues with the Transcript Request Form Owens Community College Owens, you can contact the registrar’s office for assistance. They are available to help you with any questions or concerns regarding your transcript requests.
-
Are there any benefits to using the Transcript Request Form Owens Community College Owens?
Using the Transcript Request Form Owens Community College Owens streamlines the process of obtaining your academic records. It ensures that your request is properly documented and handled efficiently, giving you peace of mind during the process.
Find out other transcript request form owens community college owens
- Close deals faster
- Improve productivity
- Delight customers
- Increase revenue
- Save time & money
- Reduce payment cycles
