
Fill and Sign the Bir 1902 Form 2008 2019
Useful suggestions for preparing your ‘Bir 1902 Form 2008 2019’ online
Are you fed up with the inconvenience of handling paperwork? Look no further than airSlate SignNow, the premier eSignature solution for individuals and organizations. Bid farewell to the tedious process of printing and scanning documents. With airSlate SignNow, you can seamlessly finalize and endorse documents online. Utilize the powerful features embedded in this user-friendly and cost-effective platform and transform your method of document management. Whether you need to endorse papers or gather electronic signatures, airSlate SignNow manages it all effortlessly, with just a few clicks.
Follow this comprehensive guide:
- Log into your account or register for a complimentary trial with our service.
- Click +Create to upload a file from your device, cloud storage, or our form repository.
- Open your ‘Bir 1902 Form 2008 2019’ in the editor.
- Click Me (Fill Out Now) to prepare the document on your end.
- Add and designate fillable fields for others (if needed).
- Continue with the Send Invite settings to request eSignatures from others.
- Save, print your copy, or convert it into a reusable template.
Don’t fret if you need to collaborate with others on your Bir 1902 Form 2008 2019 or send it for notarization—our platform provides everything you require to complete these tasks. Sign up with airSlate SignNow today and elevate your document management to new levels!
FAQs
-
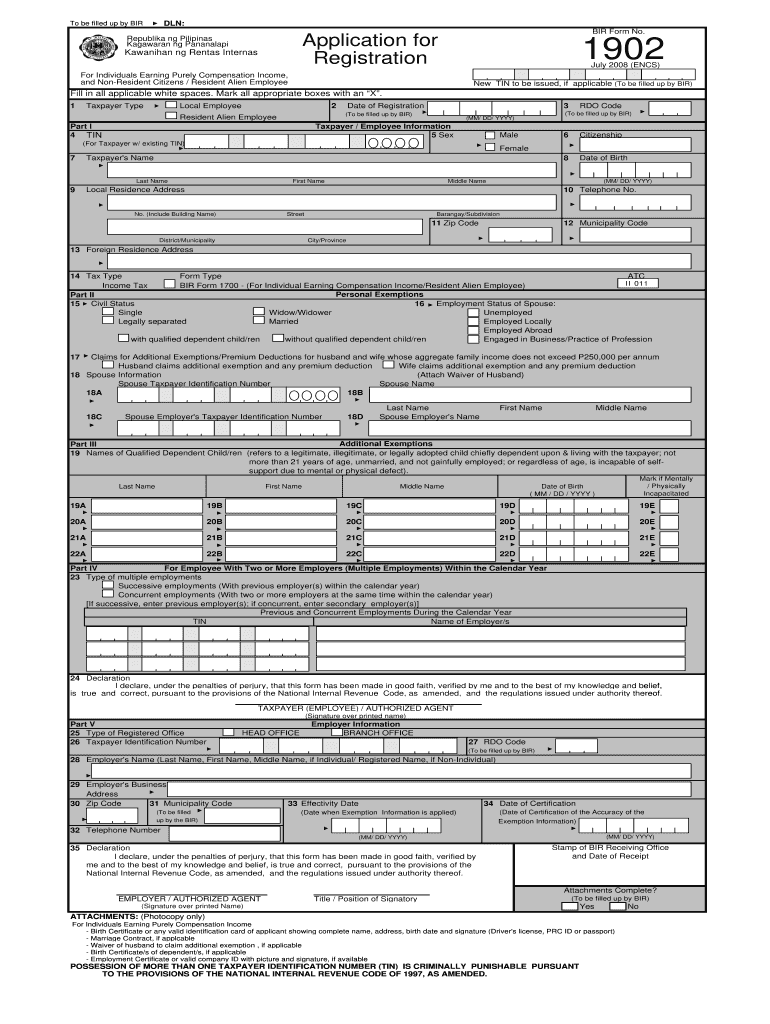
What is Bir Form 1902 and how can it be signed electronically?
Bir Form 1902 is a tax form used in the Philippines for individual income tax returns. With airSlate SignNow, you can easily fill out and eSign Bir Form 1902 online, ensuring a quick and secure submission process. The platform's intuitive interface allows you to manage your documents without hassle.
-
How does airSlate SignNow simplify the process of filling out Bir Form 1902?
airSlate SignNow streamlines the process of filling out Bir Form 1902 by providing customizable templates that eliminate the need for manual entry. Users can quickly input their information, and the platform guides them through each step, ensuring accuracy and compliance with tax regulations.
-
What are the pricing options for using airSlate SignNow to manage Bir Form 1902?
airSlate SignNow offers competitive pricing plans that cater to different business needs. Whether you're an individual or part of a larger organization, you can choose a plan that fits your budget and includes features specifically designed for managing documents like Bir Form 1902.
-
Can I integrate airSlate SignNow with other software for managing Bir Form 1902?
Yes, airSlate SignNow allows seamless integrations with popular software such as Google Drive, Dropbox, and CRM systems. This ensures that you can easily access and manage your Bir Form 1902 documents alongside your other business tools for enhanced efficiency.
-
What features does airSlate SignNow offer for securely eSigning Bir Form 1902?
airSlate SignNow provides advanced security features, including encryption and two-factor authentication, to protect your eSigned Bir Form 1902. Additionally, the platform offers audit trails, ensuring you can track all changes and signatures for compliance purposes.
-
How can airSlate SignNow enhance my team's productivity when working with Bir Form 1902?
With airSlate SignNow, your team can collaborate in real-time on Bir Form 1902, reducing the time spent on revisions and approvals. The ability to send, receive, and eSign documents electronically means faster turnaround times and increased overall productivity.
-
Is there a mobile app available for signing Bir Form 1902 on the go?
Yes, airSlate SignNow offers a mobile app that allows you to fill out and eSign Bir Form 1902 anytime, anywhere. This mobile accessibility ensures that you can manage your documents efficiently, even when you're not at your desk.
Find out other bir 1902 form 2008 2019
- Close deals faster
- Improve productivity
- Delight customers
- Increase revenue
- Save time & money
- Reduce payment cycles
