Downloaded from http://jcp.bmj.com/ on December 24, 2014 - Published by group.bmj.com
J Clin Pathol 1987;40:221-225
Serum x-thiol protease inhibitor concentrations in
health and disease
J R WEBB, E H COOPER, M A FORBES
From the Unit for Cancer Research, Medical School, University ofLeeds
Serum a-thiol protease inhibitor (a-TPI) concentration was assayed by radial immunodiffusion in normal subjects, pregnant women, and in a wide variety of diseases. The normal concentration (448 (SD 75) mg/1) increased significantly (p < 0 001) in pregnancy to 575 (89) mg/I, and in
prostatic cancer treated by oestrogens to 666 (87) mg/l. Inconsistent changes were observed in
inflammatory and malignant disease and in liver disease. A temporary pronounced fall of cx-TPI was
seen after burn injury, and a sustained fall after bone marrow transplantation. Crossed immunoelectrophoresis showed that the serum cx-TPI occurred in two forms, with a2 and al electrophoretic
mobilities. A heavy demand on this antiprotease may result in suppression of the al form.
SUMMARY
The control of proteolysis is of fundamental
importance in maintaining normal tissue function,
and the antiproteases in the blood provide a major
system to oppose the activity of a wide diversity of
proteolytic enzymes. The most widely studied in disease are the serine antiproteases, such as
oxl-antichymotrypsin
(alI-AT),
a,-antitrypsin
(@1-ACT), and a2-macroglobulin, as well as the antiproteases that regulate the clotting cascades and
fibrinolysis.1
Fundamental studies of cellular lysosomal enzymes
have identified families of proteases with specificities
other than serine. Lysosomal cysteine (thiol) proteinases have a key role in the catabolism of intracellular protein. Cathepsin B, H, and L are the most
studied enzymes of this group. Several extracellular
inhibitors specific for cysteine proteases have been
discovered, and in addition to these specific antiproteases, haptoglobin, a2-macroglobulin, IgG and
antithrombin III also inhibit cysteine proteinases.2
Serum a-thiol protease inhibitor (oa-TPI) was first
described in 1977 by Sasaki et al3 as a protein with an
a2 mobility and a molecular weight of 90 000 daltons.
In 1979 Ryley4 and Jarvinen5 both reported that TPI
isolated from human serum was not a single component but existed in two immunologically identical
forms. The main component had a molecular weight
of 90000 daltons and ran in the c2 region and the
other had an al mobility and a molecular size of
170 000-175 000 daltons. Further heterogeneity of
TPI was described recently by Sasaki et al,6 who
found three antigenically identical forms, two of
which ran in the a2 region. Antigenically active fragments of a-TPI of molecular weight 70 000 and 22 500
daltons have been found in normal human urine.7
Other inhibitors of cysteine proteinases, with lower
molecular weights (11 000- 16 000 daltons) have also
been reported,8 an example of which is cystatin, also
called y-trace protein and post-y-globulin.9
Alpha-TPI inhibits thiol proteases but does not
inhibit serine proteases, such as trypsin, chymotrypsin, or elastase. The report by Ryley4 found that
the normal serum concentration of a-TPI was 420
mg/l, with only 240 mg/l in umbilical cord serum. The
behaviour of this protein in disease has not been
examined, and in this paper we therefore looked at its
concentration in normal controls, pregnancy, and a
variety of inflammatory and malignant diseases, as
well as in advanced renal and liver disease. Alpha-TPI
was also measured in patients after severe burn injury
and after bone marrow transplantation.
Accepted for publication 6 August 1986
221
Material and methods
Serum was obtained from normal blood donors,
pregnant women, and a variety of patients, chosen to
examine the behaviour of a-TPI in malignant and
non-malignant diseases. The samples were stored at
- 20°C before their analysis.
Serum a-TPI concentrations were measured by
radial immunodiffusion,10 using antisera and standards provided by Behringwerke AG, Marburg,
�Downloaded from http://jcp.bmj.com/ on December 24, 2014 - Published by group.bmj.com
222
Lahn, West Germany. Measurements of serum Creactive protein (CRP), aI -ACT, al1-acid glycoprotein
(AGP), and steroid binding globulin (SP2) were also
made on some selected patient groups by single radial
immunodiffusion. The cx and a2 forms of TPI were
identified by crossed immunoelectrophoresis. Microheterogeneity of the glycan chains was examined by
immunoaffinoelectrophoresis using concanavalin A
in the first dimension gel, as previously described by
Wells et al."
The statistical correlations were examined by the
Wilcoxon's rank test, which is not influenced by a
skewed distribution of the analytes.
Results
The interassay coefficient of variation (CV) measured
on a control serum run in duplicate over 27 a-TPI
radial immunodiffusion plates was 9-8%.
Table 1 shows the concentrations of a-TPI found in
normal subjects, pregnant women, and in benign and
malignant diseases. There was a significant increase
(p < 0 001) in the a-TPI concentration in pregnant
women (> 6 months) and in men with prostatic
cancer receiving treatment with stilboestrol.
Of the inflammatory diseases studied, only the
patients with pneumonia and rheumatoid arthritis
showed a significant reduction (p < 0001) in the
mean a-TPI concentration. The a-TPI concentrations
in pneumonia and Crohn's disease showed no correlation with the CRP, a1-ACT, or axAGP values,
Table l Concentration of serum x-TPI in normal subjects,
pregnancy, and various diseases
Total
Mean
(SD)
Condition
no
(mg/l)
(mg/i)
Normals:
Sex unknown
Men
Women
40
23
24
466
426
439
81
53
76
40
38
446
575
84
89
40
50
40
336
470
369
70
102
59
40
38
20
463
398
442
69
110
61
43
19
39
28
12
30
37
37
421
384
378
414
506
429
666
351
93
52
63
55
109
50
87
93
Pregnancy:
< 6 months
> 6 months
Inflammatory disease:
Pneumonia
Crohn's disease
Rheumatoid arthritis
Other benign diseases:
Renal disease
Liver disease
Benign prostatic hyperplasia
Malignant disease:
Colorectal cancer
Lung cancer
Myelomatosis
Breast cancer (stages I and II)
Breast cancer (stage 111)
Prostate cancer (no treatment)
Prostate cancer (on oestrogens)
Acute leukaemia
Webb, Cooper, Forbes
indicating that TPI does not behave as an acute phase
protein.
In renal disease there was no difference between the
mean of those patients with a serum creatinine of
< 140 pmol/l (a-TPI = 455 (49) mg/l) and those with
a creatinine of > 140 pmol/l (ot-TPI = 471 (86) mg/l).
The concentrations of oc-TPI in liver disease showed
a considerable variation, as shown by the large standard deviation. There was no general tendency for the
a-TPI values to be related to a particular form, but
the lowest values were observed in portal hypertension without cirrhosis. There was no relation
between the a-TPI concentrations in liver disease and
the SP2 values, which ranged from normal, < 12, to
30 mg/I.
In malignant disease the cx-TPI measurements were
generally in the normal range, but a significant (p <
0.001) reduction in values was seen in the groups with
lung cancer, myelomatosis, and acute leukaemia.
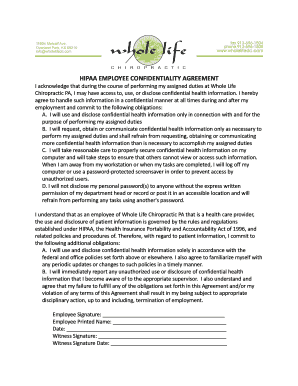
The lowest values were observed immediately following severe burn injury and in patients who had
undergone bone marrow transplantation. Figs I and
2 show that the a-TPI concentrations recovered rapidly after burn injury but remained low for several
weeks after bone marrow transplantation. Table 2
shows the mean concentrations of a-TPI in 26
patients before and after bone marrow transplantation for either acute leukaemia (myeloid and
lymphocytic) or chronic granulocytic leukaemia.
In several isolated serum samples from patients
with cancer and pregnant women no precipitin ring
on radial immunodiffusion was visible after staining.
Prolonged standing at room temperature or repeated
freezing and thawing did not affect the formation of
precipitin rings from 10 normal serum samples. If the
Fig 1 Alpha- TPI concentration after severe burn injury.
(Case I = 22%, case 2 = 57% body surface area burn.)
�Downloaded from http://jcp.bmj.com/ on December 24, 2014 - Published by group.bmj.com
223
Serum a-thiol protease inhibitor concentrations in health and disease
500
Normali meain ±2SD
o
-0
400
-
a
ep' 300.'
i _ A.
-t_
.^ o
-
- *,____-
-
Case 4
Case 3
oc-thiol protease ihibitor
oc-thiol protease inhibitor at 75 weeks 398mg/I
at 75weeks:=447mg/l
200ddCase 5
died daiy 65
100III
I
I
I
I* I
I
I
I
*
I
I
I
I
I
I
I
I
u
.I
I
I
I
4
36
32
1.0
48
4
24
28
16
20
12
4 2 4
8
Day of
Days after bone mcarrow transplantation
transplant
Fig 2 Alpha-TPI concentration after bone marrow transplantation. Cases 3 and 4 = chronic granulocytic leukaemia;
case 5 = acute myeloblastic leukaemia.
same samples were incubated for three days at 2°C at
a 1/10 dilution with a pregnancy sample which gave
no precipitin ring, however, the a-TPI was no longer
measurable by radial immunodiffusion.
there was no evidence of any accentuation of the diversity of glycan branching, as the peaks with and
without convanavalin A in the first dimension gel had
a similar appearance.
VARIATION IN THE aCl AND C2 FORMS
Discussion
Crossed immunoelectrophoresis clearly showed that
the greater part of TPI has an a2 mobility, which corresponds to the 90k monomer and the cl form of the
170k dimer is the smaller component (fig 3). Two
peaks were observed in all but one of 16 normal subjects, who exhibited only the a2 peak. In both normal
and diseased patients a double arc could often be seen
(arrows fig 3) above the area of both peaks with a
discontinuity in the precipitin line suggestive of
further microheterogeneity within this protein.
In inflammatory disease the a-TPI peak was considerably reduced and was only represented by a trace
in the burns sera. A similar result was obtained after
bone marrow transplantation. In pregnancy the peak
heights of both the a, and a2 forms were increased.
Crossed immunoaffinoelectrophoresis with concanavalin A in the first dimension gel produced only a
weak retardation of the cza and ot2 peaks. In pregnancy
Table 2 Mean (SD) a-TPI concentration (mg/l) after bone
marrow transplantation
Before
transplantation
After transplantation
4 days
366 (87)
7 days
319 (72)
(n
=
26)
(n
=
26)
28 days
348 (91)
(n = 26)
90 days
386 (95)
(n = 15)*
*There were no late follow up samples in six children. Five patients
died between 28 and 90 days, and the mean a-TPI value in these five
at 28 days was 265 (77) mg/I.
The activity of an antiprotease in the blood is
influenced by three main factors: the rate of production and release from the site of origin; the half
life of the protein in the circulation; and the rate
of removal as inhibitor-protease complexes. The
efficiency of the hepatic lectin to recognise and
capture aged molecules will depend on the lectin
recognising terminal galactose groups on the
oligosaccharide chains that are exposed after the loss
of sialic acid. Alpha-TPI contains 13% carbohydrate.4
The results of the present studies can only hint at
some of the factors that may be operating to influence
the concentrations of a-TPI in disease. The mean
a-TPI value in normal subjects (420 mg/l) agrees well
with that reported by Ryley.4 There is no difference in
the values seen in healthy men and women, but there
is a progressive rise in pregnancy, and high values can
be induced in men by oestrogens. In this respect a-TPI
responds to oestrogens in a similar fashion to a1-AT
and caeruloplasmin, both of which are increased in
pregnancy, but unlike these acute phase reactants
there is no shift in the distribution of the oligosaccharides to favour the synthesis of triantennary or
tetra-antennary chains.12 The lack of significant binding of a-TPI to concanavalin A suggests that the glycans are predominantly of the triantennary form, as it
is the biantennary forms that bind to concanavalin A
�.
Downloaded from http://jcp.bmj.com/ on December 24, 2014 - Published by group.bmj.com
224
D.
.7
iL
10%, QOPRW
IAJ-Al..
.zl.,-.,
0
.:419W
_,%
.
,k.
Webb, Cooper, Forbes
_:
....t
Fig3 Crossedimmunoelectrophoresisofserumsamples (Spl) againstantiserumtoa-TPI (l1d/cm2) inseconddimension.
a-TPI (mg/l)
Number sample
a Normal
509
b Crohn's disease (high acute phase proteins) 418
c 50 hours after severe burn injury
304
d Pregnancy 7 /2 months
578
Number sample
a-TPI (mg/l)
Prostatic cancer (no treatment)
450
f Prostatic cancer (given stilboestrol)
736
g Six days after bone marrow transplantation 217
h Stage III breast cancer
466
e
�Downloaded from http://jcp.bmj.com/ on December 24, 2014 - Published by group.bmj.com
Serum a-thiol protease inhibitor concentrations in health and disease
225
occur.
The
induction
of
by
oestrogens,
howa-TPI
and produce the microheterogeneity of the protein
that is seen in the crossed immunoaffino- ever, provides yet another example of the widespread
electrophoresis of a1-AGP and a,x-AT.'2 In chronic changes that occur in the composition of antiliver disease it could be argued there are two opposing proteases and certain acute phase reactant proteins in
factors; one being the tendency for the concentrations pregnancy, while the advantage of this change is still
of oestrogen to rise, as indicated by the induction of a matter for conjecture.
high values of steroid binding globulin (SP2), the
other being a fall in the number of hepatocytes and JRW was supported by Unipath plc, Bedford. MAF
the probable decrease in liver lectin. Clearly, the was supported by the Yorkshire Cancer Research
absence of a correlation between SP2 and a-TPI Campaign. We are grateful to Miss Cherryl Evans for
values showed that any oestrogen effect on a-TPI typing the manuscript and Ms Jill Siddall for statistical advice.
production is weak in liver disease.
In some diseases, such as pneumonia where the References
acute phase reaction is well developed, the low serum
a-TPI values may be due to an increased consumption 1 Travis J, Salvesen GS. Human plasma proteinase inhibitors. Ann
Rev Biochem 1983;52:655-709.
of this inhibitor by proteases released from inflamed
JF. Cysteine proteinase inhibitors in mammalian plasma.
cells. This may be an explanation for the low values 2 Lenney
In: Katunuma N, Umezawa H, Holzer H, eds. Proteinase
found after severe burn injury and following bone
inhibitors. Tokyo: Springer-Verlag, 1983:113-23.
marrow transplantation. The very low a-TPI concen- 3 Sasaki M, Minakata K, Yamamoto H, Niwa M, Kato T, Ito N.
A new serum component which specifically inhibits thiol protrations seen immediately after burn injury may, howteinases. Biochem Biophys Res Commun 1977;76:917-24.
ever, be due in part to loss of body fluids. Alpha-TPI 4 Ryley
HC. Isolation and partial characterisation of a thiol prowas shown to be present at about 75% of the serum
teinase inhibitor from human plasma. Biochem Biophys Res
concentration in three samples of blister fluid. The
Commun 1979;89:871-8.
values of a-TPI in advanced cancers are variable and 5 Jarvinen M. Purification and some characteristics of two human
serum proteins inhibiting papain and other thiol proteinases.
unrelated to tumour mass, which precludes it being a
FEBS Leat 1979;10B:461-4.
useful analyte to monitor or assess disease activity in 6 Sasaki
M, Taniguchi K, Minakata K. Multimolecular forms of
patients with cancer.
thiol proteinase inhibitor in human plasma. J Biochem
1981;89:169-77.
The change in the relative concentrations of the a2
K, Ito J, Sasaki M. Partial purification and properties
and a, forms seem to occur when there is a demand 7 Taniguchi
of urinary thiol proteinase inhibitors. J Biochem 1981;89:
on the system, but these were not affected by the
179-84.
hyperproduction induced by oestrogens. It cannot be 8 Turk V, Brzin J, Lenarcic B, et al. Structure and function of
lysosomal cysteine proteinases and their protein inhibitors. In:
determined whether this change in these two forms is
Intracellular protein catabolism. New York: Alan R Liss,
due to the preferential use of the dimer for anti1985:91-103.
protease activity and its removal as a complex, or 9 Simonsen
0, Grubb A, Thysell H. The blood serum concenwhether the dimerisation is inhibited. The loss of the
tration of cystatin C (y trace) as a measure of the glomerular
filtration rate. Scand J Clin Lab Invest 1985;45:97-101.
dimeric form was most noticeable shortly after severe
10 Mancini G, Carbonara AO, Heremans JF. Immunological quanburn injury when it almost disappeared.
titation of antigens by single radial diffusion. Immunochemistry
The lack of change of the serum values in renal
1965;2:235-54.
failure of neutral cysteine proteinase inhibitor, which 11 Wells C, Bog-Hansen TC, Cooper EH, Glass MR. The use of
convanavalin A crossed immuno-affinoelectrophoresis to detect
is probably identical with a-TPI, was also observed by
hormone-associated variations in a,-acid glycoprotein. Clin
Hopsu-Havu et al.`3 This is in sharp contrast to cysChim Acta 1981;109:59-67.
tatin (molecular weight 13 000 daltons), which rises 12 Raynes
J. Variations in the relative proportions of microprogressively as the glomerular filtration rate falls.'3
heterogenous forms of plasma glycoproteins in pregnancy and
disease. Biomedicine 1982;36:77-86.
The half lives of the two principal molecular size
A, Jarvinen M,
forms of a-TPI will differ considerably, as like the 13 Hopsu-Havu VK, Joronen I, Havu S, Rinne
Forsstrom J. Serum cysteine proteinase inhibitors with special
larger glycoproteins, they are in the range of four to
reference to kidney failure. Scand J Clin Lab Invest 1985;4S:
eight days, whereas low molecular weight proteins,
11-6.
such as f2-microglobulin (molecular weight 11 300 14 Vincent C, Pozet N, Revillard JP. Plasma f2-microglobulin turnover in renal insufficiency. Acta Clin Beig 1980;35(10):2-13.
daltons), have half lives of about one hour.'4
This survey has raised several questions about the
factors controlling the serum concentrations of this Requests for reprints to: Professor EH Cooper, The Unit for
form of antiprotease and has shown several condi- Cancer Research, School of Medicine, The University of
tions in which prolonged depletion of a-TPI may Leeds, Leeds LS2 9NL, England.
�Downloaded from http://jcp.bmj.com/ on December 24, 2014 - Published by group.bmj.com
Serum alpha-thiol protease
inhibitor concentrations in health
and disease.
J R Webb, E H Cooper and M A Forbes
J Clin Pathol 1987 40: 221-225
doi: 10.1136/jcp.40.2.221
Updated information and services can be found at:
http://jcp.bmj.com/content/40/2/221
Email alerting
service
Receive free email alerts when new articles cite this
article. Sign up in the box at the top right corner of the
online article.
Notes
To request permissions go to:
http://group.bmj.com/group/rights-licensing/permissions
To order reprints go to:
http://journals.bmj.com/cgi/reprintform
To subscribe to BMJ go to:
http://group.bmj.com/subscribe/
�