Thorax 1985;40:459-464
A self paced treadmill walking test for breathless
patients
A BEAUMONT, A COCKCROFT, A GUZ
From the Department of Medicine, Charing Cross and Westminster Medical School, London
ABSTRACT A treadmill exercise test is described that retains the advantages of self paced walking
but allows the measurement of cardiorespiratory variables. A horizontal treadmill was modified
to allow patients to control their own speed. During exercise continuous measurements of speed,
distance, heart rate, arterial oxygen saturation, and stride length were made and subjective
assessments of breathlessness were recorded on a visual analogue scale. Ten men with severe
chronic obstructive lung disease performed a 12 minute corridor walk and a self paced 12 minute
treadmill walk on the same day and repeat treadmill walks on different days. Six of them
performed three walks or more. Six patients had ventilatory measurements during treadmill
exercise. There was no significant difference (p > 0.1) in the distance covered during corridor and
treadmill walks, and distances on the treadmill were repeatable after the first walk. Use of a
mouthpiece significantly reduced the distance covered on the treadmill. The self paced treadmill
walk is a simple repeatable test and has advantages over both a corridor walking test and standard
progressive tests for assessment of breathless patients.
A 12 minute exercise test was originally described
by Cooper' as an indication of physical fitness in
young normal subjects. He found a close correlation
between the distance run in 12 minutes and the
maximum oxygen uptake measured on a treadmill.
McGavin and coworkers2 modified the 12 minute
exercise test for patients with chronic obstructive
lung disease. They asked patients to cover as much
distance as they could in 12 minutes along a level
hospital corridor and they found this to be a reproducible index of exercise tolerance.2 The reproducibility of the 12 minute walking distance has been
confirmed by others.34
The major disadvantage of this type of corridor
walking test is the lack of information about
physiological and symptomatic changes during exercise. Monitoring these changes is important when
studying mechanisms of exercise limitation and
when investigating the effects of exercise training
programmes in disabled patients.
Our study was undertaken to develop and validate
a self paced treadmill walking test, which was similar
to the 12 minute corridor walking test in that
patients were in complete control of their speed, but
which allowed measurements of physiological variables during the exercise. The treadmill walk was
validated in two ways: by comparison with the
results of a corridor walk performed on the same
day and by comparison of the results of repeated
treadmill walks on different days. The work has
already been presented in preliminary form.5
Methods
SUBJECTS
We studied 10 men aged 46-73 years. All had
chronic airways obstruction, with mean forced
expiratory volume in one second (FEV,) of 1.03
(SD 0.27, range 0.54-1.39) 1 and mean forced vital
capacity (FVC) of 2.68 (SD 0.60, range 1.6-3.74)1.
Two women were also tested in the comparison of
treadmill walks with and without a mouthpiece
(FEV, 0.8, FVC 2.3; FEV, 0.6, FVC 2.3 1).
PROTOCOL
Address for reprint requests: Dr A Cockcroft, Department of
Medicine, Charing Cross and Westminster Medical School, London
W6 8RF.
Accepted 2 January 1 985
Spirometry was performed in all patients on the days
of exercise testing. The 10 men performed a standardised 12 minute corridor walk along a level hospital corridor and a treadmill walk on the same day,
459
�460
in random order. A minimum of 45 minutes' rest
was allowed between the two exercises. All 10
patients completed a second treadmill walk on a different day and six of them performed a third treadmill walk. Six patients (four of the men and the two
women) had ventilatory measurements made during
the treadmill walk with a mouthpiece and
pneumotachograph and this walk was compared
with a control treadmill walk performed on the same
day.
THE CORRIDOR WALK
The corridor walk was carried out as described by
McGavin et al.2 The patients were instructed to walk
as far as they could in 12 minutes; they were told to
keep going if possible but they could slow down or
even stop if necessary. An operator accompanied
each patient to record distance and time, and to give
encouragement with standard phrases. The number
of right heel strikes over 40 m distances was
recorded for calculation of stride length.
THE TREADMILL WALK
The treadmill walk was performed on a horizontal
treadmill (Marquette Electronics Ltd, USA) fitted
with a remote control module modified for the
patient's use. This comprised four easily accessible
push buttons that allowed the treadmill to be stopped, started, speeded up, or slowed down. Stopping
and changing speed occurred gradually, with acceleration or deceleration of 100 m min 2; starting,
although abrupt, was always from the slowest speed
(1.5 km/h) and with the operator's assistance.
Patients practised walking on the treadmill before
starting the 12 minute walk. Standardised instructions and encouragement similar to those for the
corridor walk were given during the exercise via a
tape recording. Patients were instructed to walk "as
far as possible" during the time-that is, as fast as
possible. They were told that they could slow down
or even stop if necessary. During the test the voltage
output of speed from the treadmill was fed into a
Mini analogue computer (AEI, USA), which integrated the signal to give a voltage output of distance.
Stride length was derived by the analogue computer: the number of right heel strikes recorded by a
pedometer was divided into distance covered every
30 seconds. The pedometer consisted of a calculator
keyboard switch taped into the right shoe under the
heel. These signals were recorded continuously on a
Mingograf strip chart recorder (Siemens, Holland).
Arterial oxygen saturation was monitored at rest
and throughout the exercise with a spectrophotometric ear oximeter6 (Hewlett Packard,
USA). Heart rate and electrocardiogram were monitored throughout.
Beaumont, Cockcroft, Guz
Subjective assessments of breathlessness were
recorded during the treadmill walk on a visual
analogue scale.' The patients were presented with a
10 cm visual display on which a red light could be
positioned by a linear sliding potentiometer. The left
end of the scale was labelled "not at all breathless"
and the right end "extremely breathless." Patients
were asked to signal at the moment when they first
felt breathless and then to indicate how breathless
they felt on the visual analogue scale every 30 seconds, prompted by a light signal. A mean breathlessness score was obtained by summing all the
scores during the test and dividing by 24 (the
number of half minute periods); this has been used
as an index of overall breathlessness.
The six patients in whom ventilatory measurements were made during the treadmill walk
breathed through a pneumotachograph (Fleisch No
1 or 2) attached to a Fenyves and Gut Ergostar8
(Basel, Switzerland). Mixed expired gas was analysed for carbon dioxide and oxygen; and carbon
dioxide production, oxygen consumption, and ventilation were calculated over half minute periods. All
equipment was calibrated before every exercise test.
ANALYSIS
Corridor and treadmill walking distances were compared by means of a paired t test. Repeatability of
the treadmill walk was assessed by comparing distances covered in each quarter of the time for separate walks; paired t tests were used to compare
three, six, nine, and 12 minute distances for walks 1
and 2, and 2 and 3.
Results
Most patients found the treadmill walk acceptable
and had no difficulty controlling treadmill speed.
Training patients to walk normally on the treadmill
was accomplished fairly easily. All patients but one
experienced some reduction in oxygen saturation
during the treadmill exercise, with a maximum fall
of 18% (from 92% to 74%). No patient complained
of chest pain during the tests but ST segment depression consistent with ischaemic heart disease was
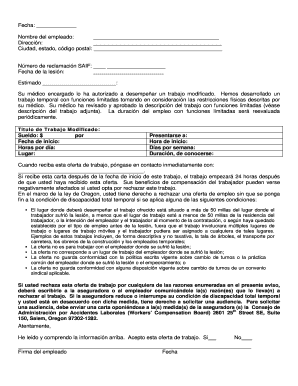
noted in one patient. Figure 1 is shown as an example of the sort of information that can be obtained
during a treadmill walk. In this particular patient
increases in speed were accompanied by increases in
the visual analogue scale score for breathlessness at
a constant level of oxygen saturation.
COMPARISON OF TREADMILL AND CORRIDOR
WALKS
The 10 men who performed both corridor and
�A self paced treadmill walking test for breathless patients
461
treadmill walks said that walking on the treadmill (fig 3). Two patients stopped walking during one or
was almost as easy as walking in the corridor. The both of the tests; both stopped more frequently in
relationship of stride length to walking speed the corridor.
seemed similar for corridor and treadmill walks (fig
2). The distance walked on the treadmill was not REPEATABILITY OF TREADMILL WALKS
significantly different (p > 0.1) from that covered in The distance covered during the first treadmill walk
the corridor on the same day by the group as a whole was significantly shorter than that covered during
the second (n = 10, p < 0.05: fig 4). For the patients
who completed three or more treadmill walks, there
100 r
was no significant difference between the second
and third walking distances (n = 6, p > 0.1, fig 5); in
this subgroup there was also no significant difference
between the first and second walking distances (p >
E 700
0.1), and this presumably reflects the reduced size of
the subgroup. Despite the greater distance (and
500
speed) of the second treadmill walk, the mean score
._A
Ci
for breathlessness assessed by visual analogue scale
was not different from that recorded during the first
300
treadmill walk (p > 0.2). Similarly, breathlessness
scores did not differ between the second the third
100
treadmill walks (p > 0.4).
Patients differed in the way they achieved their
8
total 12 minute distance on the treadmill: some
walked at a steady pace throughout, while others
varied their speed during the test. For individual
6
E
patients the pattern was relatively constant: when
the second and third treadmill walks were com4
pared, the distances covered over consecutive three
minute periods of the tests did not differ significantly
2_
between tests (six men).
Q
oJ
I
I
I
EFFECT OF THE MOUTHPIECE AND
PNEUMOTACHOGRAPH
Treadmill walking distance was less, for five out of
six patients when they performed the test with a
mouthpiece and heated pneumotachograph (Fleisch
No 2-dead space 55 ml) than during a control walk
(fig 6). The difference in distance covered was
significant (p < 0.05). Mean visual analogue scale
scores for the control walk (mean 25.8 (SD 24.5))
and the walk with a mouthpiece (mean 27.8 (23.8))
were not significantly different (p > 0.4). Patients
reported that the mouthpiece made the treadmill
walk more unpleasant.
95
Discussion
85
These results suggest that the 12 minute self paced
treadmill walk can be used for physiological evaluation during exercise of patients disabled by breathlessness. The similar distances covered by patients
on the treadmill and in the corridor, and the fact that
the relation of stride length and speed was apparently the same for the two types of walk, suggests
that patients were walking on the treadmill in the
same way as in the corridor.
c
a
v
iG
a
0
2
4
6
8
10
12
Time (mini
Fig I A selfpaced 12 minute treadmill walk with
continuous measurements of distance, speed, and arterial
oxygen saturation. Subjective breathlessness was scored on a
visual analogue scale (VAS).
�462
The treadmill walking distance was repeatable
after the first walk. We now use the first treadmill
walk as a training procedure, in common with other
investigators who have used the corridor walk. Not
only was the total distance repeatable after the first
treadmill walk but intermediate three minute distances were remarkably consistent for individual
subjects, suggesting that each had their own "best
way" of covering the greatest distance in the time.
Interestingly, the mean breathlessnes score for the
second treadmill walk was the same as for the first,
despite the greater distance on the second occasion.
This could mean that the patients were limiting
themselves at the same symptomatic level on the
two occasions; the lesser breathlessness relative to
speed on the second occasion is unexplained.
The treadmill walking test allows measurements
of gas exchange to be made during exercise, which
may be important in studies of the mechanisms that
limit exercise tolerance in patients with chronic obstructive lung disease. This, however, requires the
patient to breathe through a mouthpiece and
pneumotachograph, which we found significantly
reduced the distance walked. Visual analogue scale
scores were not reduced despite the shorter distance
covered when a mouthpiece was used, again suggesting that patients were limiting themselves at a given
level of breathlessness. In view of this effect of the
mouthpiece and pneumotachograph, it is clearly
reasonable to compare walking distances on the
treadmill only if they are performed in similar cir-
Beaumont, Cockcroft, Guz
cumstances (that is, with or without a mouthpiece)
in studies of the effects of, for example, exercise
training. Other variables that are difficult to measure during corridor walking but can easily be meas4-
1200 r
E
4Il)
C
1000 F
/6/
800 k
*_
0
,/
/~~~~~~~~~
"
i 6001
*_
//e
r-
to
L.rE:
as
/
200 F
/
I
I
I
I
Fig 3 Comparison of 12 minute corridor walking distance
for 1O patients with selfpaced 12 minute treadmill walking
distance performed on the same day, in random order.
Mean treadmill distance = 742 (SD 224) m; mean corridor
distance = 791 (224) m; SD of difference = 100 m (p >
0.1); r = 0.898, slope = 0.895, intercept = -33.4 m. The
dashed line is the line of identity.
U
*
0.6 p
a
0
MC
a
CD
c
50)
0.4
4)
0.2 u
I
l
200 400 600 800 1000 1200
Corridor walking distance (m)
0.8 r
S
E
~
4001
I
I
I
I
I
I
1
2
3
4
5
6
Speed (km/h)
Fig 2 Relationship between average stride length and speed for corridor
(over 40 m distance) and treadmill (over 30 second period) walking; pauses
are not included. Each of the 10 patients is represented by a different
symbol; open symbols are for corridor measurements, closed symbols for
the treadmill. For some patients more than one point of comparison between
stride length and speed was possible for either treadmill or corridor walking
and all points are shown.
�A selfpaced treadmill walking test for breathless patients
463
ured during the treadmill walk incluc11le EzLC G2
configuration, assessments of breathlessn(ezss on a '- 1200
visual analogue scale during the exercise, a],rnd arter- @
ial oxygen saturation measured by ear oximiteter. It is 0 ° 1000.
even possible to sample from an arterial lirIe during tno
4
the treadmill walk.9
This type of exercise test may have ad11Ivantages c
800
I
w
_-
le,
-
-V
1200
-
,
1000
9-a
_-3
/
4J)
.(A
-E
0
*/
B
0.
,S
600
xX
3
--l
C
//
//0~~~
4
400
-
/
.
r 800
0 0
C
`
F
600
0
39
o 200
EC
0'i
F
L 200
+j
la
4.)w
L
400
-
I
I
I
I
I
II
I
C_
200 400 600 800 1000 1200
1st treadmill walking distance (m)
Fig 4 Comparison of distance walked on the treadmill on
the first and second occasions for 10 patients. First walk:
mean distance = 712 (SD 203) m; second walk: mean
distance = 758 (221) m; SD of difference = 58 m (p <
0.05); r = 0.'964, slope = 1.051 intercept = 11.1 m. The
dashed line is the line of identity.
E 1200
0
4.)
_ 800
C
-I
600
cm
3:
r-400
w
0
CE
200
4.)
Li
la,
O0
I
I
I
a
I
200 400 600 800 1000 1200
12 min treadmill walking distance (im)
Fig 6 Effect of mouthpiece and pneumotachograph on 12
minute treadmill walking distance for six patients. Control
walk: mean distance = 658 (SD 273) m; "mouthpiece
walk" mean distance = 547 (251) m; SD of difference
= 117 m (p < 0-05); r = 0-960, slope = 0*885, intercept
=
-
35-2 m. The dashed line is the line of identity.
over the standard progressive respiratory exercise
test,'" on bicycle or treadmill in very disabled
patients. Such patients find progressive tests frightening and unpleasant and often can exercise only for
very short periods, producing limited data for
analysis. More information is available from a
longer, self paced test. Measurements at the time of
stopping and restarting exercise, or with voluntary
changes in speed, may be of particular value in
assessing factors limiting everyday activity. This
information is not obtained during a progressive
test. Thus a self paced treadmill walk may be better
than either a corridor walking test or a standard
progressive test for assessing severely breathless
patients. So far we have formally assessed the test
only for patients disabled by respiratory disease but
preliminary work suggests that it will also be useful
in the assessment of patients disabled by breathlessness and fatigue due to poor left ventricular function.
We thank Dr Lewis Adams for much helpful discus200 400
600 800 1000 1200
sion.
2nd treadmill walking distance (m)
Fig 5 Comparison of distance walked on the treadmill on
the second and third occasions for six patients. Second walk: References
mean distance = 751 (SD 261) m; third walk: mean
distance = 788 (273) m; SD of difference 56 m
1 Cooper KH. A means of assessing maximal oxygen
(p > 0.1); r = 0-979, slope = 1 027, intercept 17-6 m.
intake. JAMA 1968;203:201-4.
The dashed line is the line ofidentity.
2 McGavin CR, Gupta SP, McHardy GJR. Twelve
=
=
�Beaumont, Cockcroft, Guz
464
3
4
5
6
minute walking test for assessing disability in chronic
bronchitics. Br Med J 1976;i:822-3.
Mungall IPF, Hainsworth R. Assessment of respiratory
function in patients with chronic obstructive airways
disease. Thorax 1979;34:254-8.
O'Reilly JF, Shaylor JM, Fromings KM, Harrison
BDW. The use of the 12 minute walking test in assessing the effect of oral steroid therapy in patients with
chronic airways obstruction. Br J Dis Chest 1982;
76:374-82.
Beaumont A, Cockcroft A, Guz A. A treadmill walking test for breathless patients. Clin Sci 1983;64: 11P
(abstract).
Saunders NA, Powles ACP, Rebuck AS. Ear oximetry:
Accuracy and practicability in the assessment of arter-
ial oxygenation. Am Rev Respir Dis 1976;113:745-9.
7 Adams L, Chronos N, Lane R, Guz A. The measurement of breathlessness induced in normal subjects:
validity of two scaling techniques. Clin Sci
1985;69:7-16.
8 Reinhard U, Muller PH, Schmulling RM. Determination of anaerobic threshold by the ventilation equivalent in normal individuals. Respiration 1979;38:36-42.
9 Cockcroft A, Beaumont AG, Adams L, Guz A.
Arterial oxygen desaturation during treadmill and
bicycle exercise in patients with chronic obstructive
airways disease. Clin Sci 1985;68:327-32.
10 Jones NL, Campbell EJM. Clinical exercise testing. 2nd
ed. Philadelphia: WB Saunders, 1982.
�