
Fill and Sign the State of Arizona Assignment of Trade Name Application Form
Useful advice on preparing your ‘State Of Arizona Assignment Of Trade Name Application Form’ online
Are you fed up with the inconvenience of managing paperwork? Look no further than airSlate SignNow, the premier electronic signature solution for both individuals and organizations. Bid farewell to the monotonous process of printing and scanning documents. With airSlate SignNow, you can effortlessly complete and sign documents online. Utilize the robust features integrated into this intuitive and affordable platform and transform your approach to document management. Whether you need to approve forms or gather signatures, airSlate SignNow manages it all seamlessly with just a few clicks.
Follow this step-by-step guide:
- Sign in to your account or register for a free trial with our service.
- Click +Create to upload a document from your device, cloud storage, or our form library.
- Open your ‘State Of Arizona Assignment Of Trade Name Application Form’ in the editor.
- Click Me (Fill Out Now) to prepare the document on your end.
- Add and designate fillable fields for others (if needed).
- Proceed with the Send Invite settings to request eSignatures from others.
- Save, print your version, or convert it into a reusable template.
Don’t fret if you need to work with others on your State Of Arizona Assignment Of Trade Name Application Form or send it for notarization—our solution provides everything you need to complete such tasks. Create an account with airSlate SignNow today and enhance your document management to a new level!
FAQs
-
What is the State Of Arizona Assignment Of Trade Name Application Form?
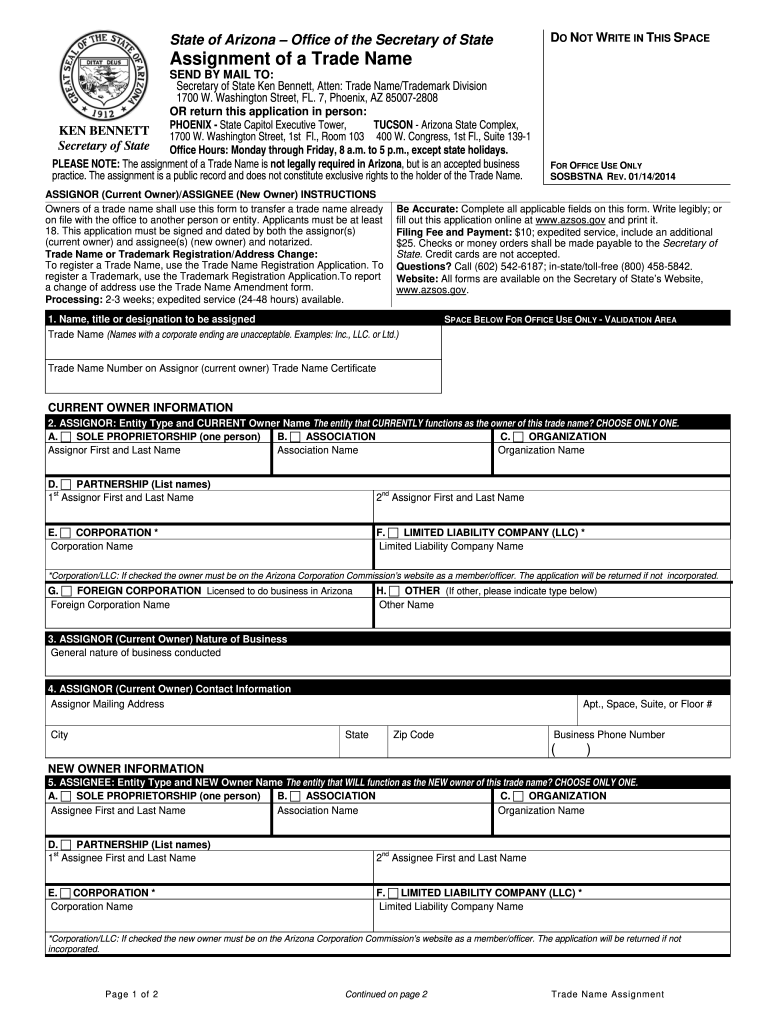
The State Of Arizona Assignment Of Trade Name Application Form is a legal document used to transfer the rights to a trade name from one entity to another. This form is essential for businesses looking to maintain brand continuity while changing ownership or structure. Completing this form correctly ensures that your trade name remains protected under Arizona law.
-
How do I complete the State Of Arizona Assignment Of Trade Name Application Form using airSlate SignNow?
Completing the State Of Arizona Assignment Of Trade Name Application Form with airSlate SignNow is straightforward. Our platform offers an intuitive interface that allows you to fill out the form digitally, ensuring all necessary information is included. Once completed, you can easily eSign the document and send it for approval.
-
Is there a fee to file the State Of Arizona Assignment Of Trade Name Application Form?
Yes, there is typically a fee associated with filing the State Of Arizona Assignment Of Trade Name Application Form. The exact amount may vary based on the specific requirements of your application. It's advisable to check with the Arizona Secretary of State's office for the most current fees and payment options.
-
What are the benefits of using airSlate SignNow for the State Of Arizona Assignment Of Trade Name Application Form?
Using airSlate SignNow for the State Of Arizona Assignment Of Trade Name Application Form streamlines the process, making it faster and more efficient. Our platform allows for easy document management and ensures that all signatures are legally binding. Additionally, you can access your documents anytime, anywhere, enhancing your workflow.
-
Can I integrate airSlate SignNow with other business tools for managing the State Of Arizona Assignment Of Trade Name Application Form?
Absolutely! airSlate SignNow offers integrations with various business tools, enabling seamless management of your documents, including the State Of Arizona Assignment Of Trade Name Application Form. Whether you use CRM systems or project management software, our integrations help streamline your processes and improve efficiency.
-
What features does airSlate SignNow provide for handling the State Of Arizona Assignment Of Trade Name Application Form?
airSlate SignNow provides several features to assist with the State Of Arizona Assignment Of Trade Name Application Form, including customizable templates, automated workflows, and secure eSignature options. These features ensure that you can complete and submit your forms quickly while maintaining compliance with legal standards.
-
How secure is the airSlate SignNow platform for submitting the State Of Arizona Assignment Of Trade Name Application Form?
Security is a top priority at airSlate SignNow. When submitting the State Of Arizona Assignment Of Trade Name Application Form, your data is protected with advanced encryption protocols and compliance with industry standards. This ensures that your sensitive information remains safe throughout the signing process.
Find out other state of arizona assignment of trade name application form
- Close deals faster
- Improve productivity
- Delight customers
- Increase revenue
- Save time & money
- Reduce payment cycles
