
Fill and Sign the California Sales and Use Tax Certificate Form
Valuable tips for finalizing your ‘California Sales And Use Tax Certificate Form’ online
Are you fed up with the inconvenience of managing paperwork? Look no further than airSlate SignNow, the premier eSignature tool for both individuals and businesses. Bid farewell to the lengthy process of printing and scanning documents. With airSlate SignNow, you can easily complete and sign forms online. Take advantage of the powerful features included in this intuitive and affordable platform and transform your document management strategy. Whether you need to approve documents or collect eSignatures, airSlate SignNow takes care of everything seamlessly, with just a few simple clicks.
Adhere to this comprehensive guide:
- Access your account or register for a complimentary trial with our service.
- Select +Create to upload a file from your device, cloud storage, or our template library.
- Open your ‘California Sales And Use Tax Certificate Form’ in the editor.
- Click Me (Fill Out Now) to set up the document on your end.
- Add and designate fillable fields for others (if necessary).
- Proceed with the Send Invite options to obtain eSignatures from others.
- Save, print your version, or convert it into a reusable template.
Don’t fret if you need to collaborate with your team on your California Sales And Use Tax Certificate Form or send it for notarization—our solution provides all the tools required to achieve those tasks. Register for an account with airSlate SignNow today and elevate your document management to new levels!
FAQs
-
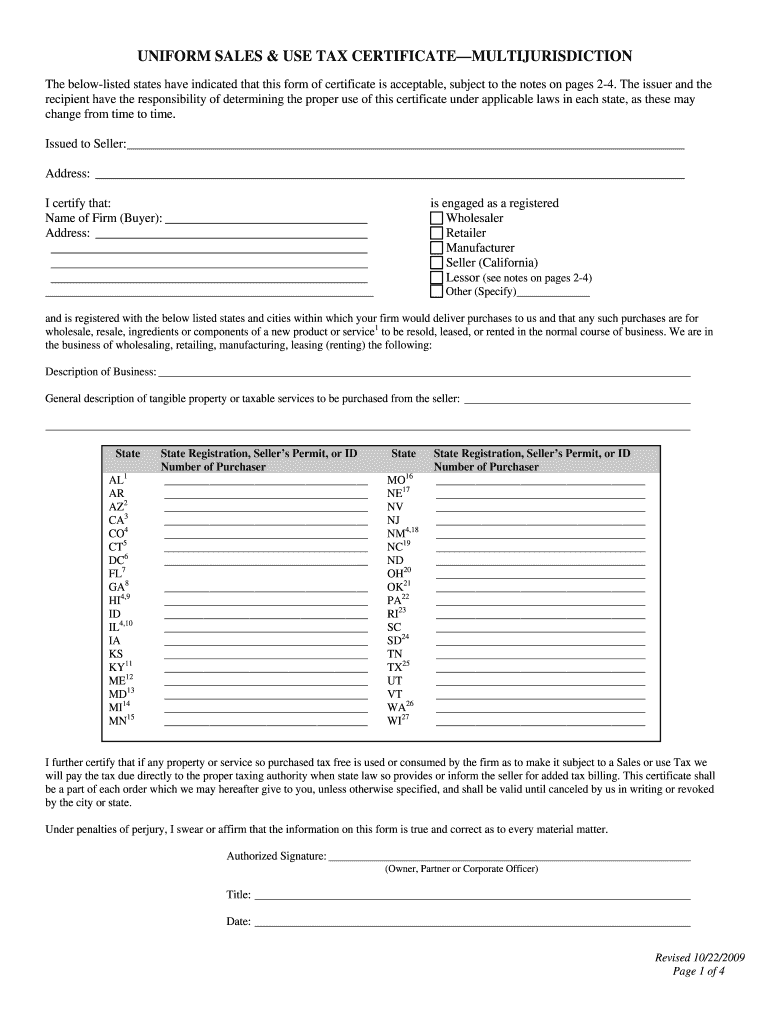
What is the California Sales And Use Tax Certificate Form?
The California Sales And Use Tax Certificate Form is a legal document that allows businesses in California to purchase goods without paying sales tax. This form is essential for retailers who wish to sell taxable items and need to provide proof of their tax-exempt status. By using this certificate, businesses can streamline their tax processes and comply with California tax regulations.
-
How can airSlate SignNow help me with the California Sales And Use Tax Certificate Form?
airSlate SignNow provides an efficient platform for businesses to create, send, and eSign the California Sales And Use Tax Certificate Form quickly. Our user-friendly interface ensures that you can complete and manage your forms effortlessly, saving time and reducing paperwork. With airSlate SignNow, you can focus on your business while we handle your document needs.
-
Is there a cost associated with using airSlate SignNow for the California Sales And Use Tax Certificate Form?
Yes, airSlate SignNow offers various pricing plans to suit different business needs. Depending on the features and number of users, you can choose a plan that includes access to the California Sales And Use Tax Certificate Form and other essential document management tools. We aim to provide a cost-effective solution for all your eSignature needs.
-
Can I integrate airSlate SignNow with other software for managing the California Sales And Use Tax Certificate Form?
Absolutely! airSlate SignNow seamlessly integrates with popular applications such as Salesforce, Google Drive, and Dropbox, enhancing your ability to manage the California Sales And Use Tax Certificate Form. These integrations allow you to streamline your workflow and access your documents in one place, making it easier to stay organized.
-
What are the benefits of using airSlate SignNow for the California Sales And Use Tax Certificate Form?
Using airSlate SignNow for the California Sales And Use Tax Certificate Form comes with numerous benefits, including enhanced security, ease of use, and quicker turnaround times. Our platform ensures that your documents are securely stored and can be accessed anytime, boosting your team's productivity. Plus, eSigning is fast and legally binding, making compliance easier.
-
How secure is my information when using airSlate SignNow for the California Sales And Use Tax Certificate Form?
Security is a top priority at airSlate SignNow. When you use the California Sales And Use Tax Certificate Form, your information is protected by industry-standard encryption and secure servers. We are committed to keeping your documents safe and confidential, giving you peace of mind as you manage important business paperwork.
-
Can I customize the California Sales And Use Tax Certificate Form with airSlate SignNow?
Yes! airSlate SignNow allows you to customize the California Sales And Use Tax Certificate Form to meet your specific business needs. You can add branding elements, modify fields, and tailor the document layout, ensuring that it reflects your company's identity while still complying with California tax regulations.
Find out other california sales and use tax certificate form
- Close deals faster
- Improve productivity
- Delight customers
- Increase revenue
- Save time & money
- Reduce payment cycles
