
Fill and Sign the Workers Compensation Disputed Claim for Compensation Form
Useful suggestions for preparing your ‘Workers Compensation Disputed Claim For Compensation Form ’ online
Are you fed up with the inconvenience of handling paperwork? Look no further than airSlate SignNow, the premier eSignature solution for individuals and small to medium-sized businesses. Wave goodbye to the lengthy procedure of printing and scanning documents. With airSlate SignNow, you can effortlessly finalize and sign documents online. Leverage the robust features packed into this intuitive and cost-effective platform and transform your approach to document management. Whether you need to sign documents or gather electronic signatures, airSlate SignNow manages it all seamlessly, with just a few clicks.
Follow this step-by-step guide:
- Sign in to your account or sign up for a complimentary trial with our service.
- Click +Create to upload a file from your device, cloud storage, or our template library.
- Open your ‘Workers Compensation Disputed Claim For Compensation Form ’ in the editor.
- Click Me (Fill Out Now) to prepare the document on your end.
- Add and designate fillable fields for other participants (if required).
- Proceed with the Send Invite settings to solicit eSignatures from others.
- Download, print your copy, or convert it into a multi-usable template.
No need to worry if you need to collaborate with others on your Workers Compensation Disputed Claim For Compensation Form or send it for notarization—our platform provides everything necessary to accomplish such tasks. Sign up with airSlate SignNow today and elevate your document management to new levels!
FAQs
-
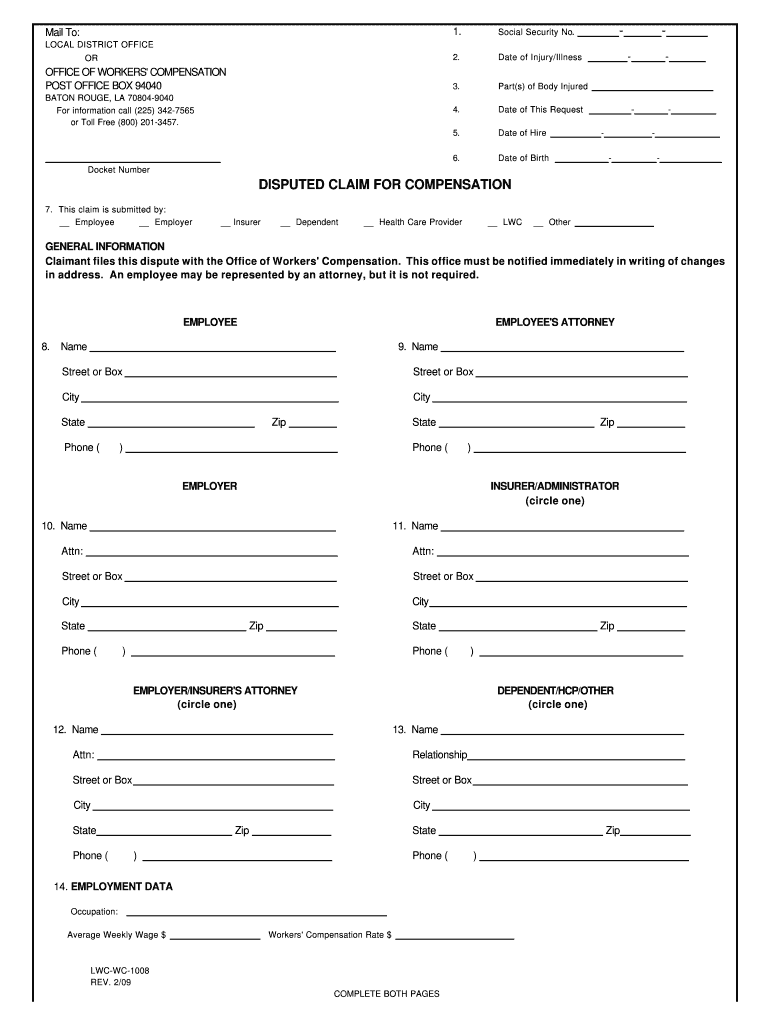
What is the Workers' Compensation Disputed Claim For Compensation Form?
The Workers' Compensation Disputed Claim For Compensation Form is a crucial document used when an employee disputes a workers' compensation claim. It allows both parties to formally outline the disagreement and initiate the necessary processes to resolve the issue. With airSlate SignNow, you can easily create, send, and eSign this form, ensuring a smooth and efficient workflow.
-
How can airSlate SignNow help with the Workers' Compensation Disputed Claim For Compensation Form?
airSlate SignNow streamlines the process of managing the Workers' Compensation Disputed Claim For Compensation Form by providing a user-friendly platform for creating and signing documents. Our solution ensures that all parties can easily review, eSign, and track the status of the form, reducing delays and improving communication. This efficiency can signNowly benefit both employers and employees during disputes.
-
Is there a cost associated with using airSlate SignNow for the Workers' Compensation Disputed Claim For Compensation Form?
Yes, airSlate SignNow offers various pricing plans to accommodate different business needs. Each plan includes features that facilitate the management of documents like the Workers' Compensation Disputed Claim For Compensation Form, ensuring you have the tools necessary for an effective claims process. You can choose a plan that best fits your budget and requirements.
-
What features does airSlate SignNow offer for managing the Workers' Compensation Disputed Claim For Compensation Form?
airSlate SignNow offers a range of features designed to enhance the management of the Workers' Compensation Disputed Claim For Compensation Form. These include customizable templates, eSignature capabilities, document tracking, and secure cloud storage. These features make it easy to create, send, and manage your claims efficiently.
-
Can I integrate airSlate SignNow with other tools for processing the Workers' Compensation Disputed Claim For Compensation Form?
Absolutely! airSlate SignNow offers seamless integrations with various tools and platforms, allowing you to enhance your workflow for the Workers' Compensation Disputed Claim For Compensation Form. Whether you're using project management software or HR systems, our integrations help streamline the claims process and improve efficiency.
-
What are the benefits of using airSlate SignNow for the Workers' Compensation Disputed Claim For Compensation Form?
Using airSlate SignNow for the Workers' Compensation Disputed Claim For Compensation Form offers several benefits, including increased efficiency, reduced processing time, and improved accuracy. Our platform simplifies document management, allowing both employers and employees to focus on resolving disputes rather than getting bogged down in paperwork.
-
Is airSlate SignNow easy to use for the Workers' Compensation Disputed Claim For Compensation Form?
Yes, airSlate SignNow is designed with user-friendliness in mind, making it easy for anyone to navigate the platform and handle the Workers' Compensation Disputed Claim For Compensation Form. With an intuitive interface and straightforward features, you can quickly create and eSign documents without extensive training.
Find out other workers compensation disputed claim for compensation form
- Close deals faster
- Improve productivity
- Delight customers
- Increase revenue
- Save time & money
- Reduce payment cycles
